
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
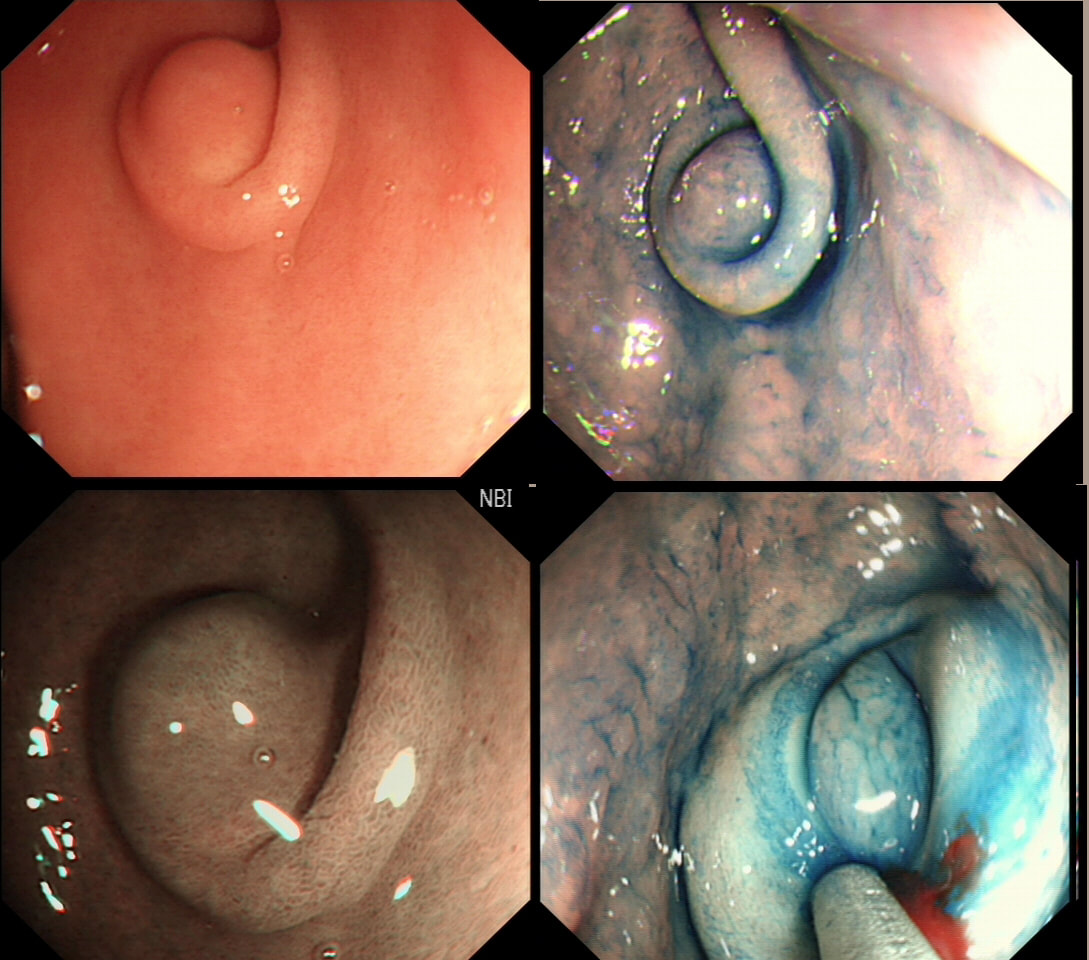
This antral lesion was found in a 25 yr old man undergoing gastroscopy for dyspepsia. Surface biopsies have only revealed a normal gastric mucosa.
WHAT WOULD YOU ADVICE?
explanation
This is a typical appearance of an 'ectopic pancreas' in the classical location along the greater curve of the antrum. The lesion even has a central dimple where the pancreatic duct finishes and a beautiful fold draped around it (which may not always be present in these lesions of course).
Sometimes I am asked to remove these for the 'reassurance' or to obtain a 'definite diagnosis' or because it's causing pain. Pain due to pancreatitis arising in these has been reported but is probably less common than finding that the rocking horse has shat on the floor. When the endoscopic appearances are typical, I don't believe that any further 'confirmation' is necessary. At Gastroscopy, I report these as: "small pancreatic rest was noted in the antrum. This is a normal, incidental finding of no significance" If you foolishly try to remove these, you will find that the endoscopic resection is actually quite difficult. The central pancreatic duct tethers the lesion down and therefore these never elevate well. You can see that in the bottom row image on the right. After struggling, you will end up with a mucosal defect and a central pink area (see image below). The resected fragments will only contain normal gastric mucosa and you will have to either dig deeper (have you heard of the expression: "to dig an even deeper hole for yourself?") or take some samples from the central pink area to capture some pancreatic duct tissue. If the referring team are steadfast that "proof is needed that the lesion is innocent", an EUS is safer and easier than an attempt at endoscopic resection. 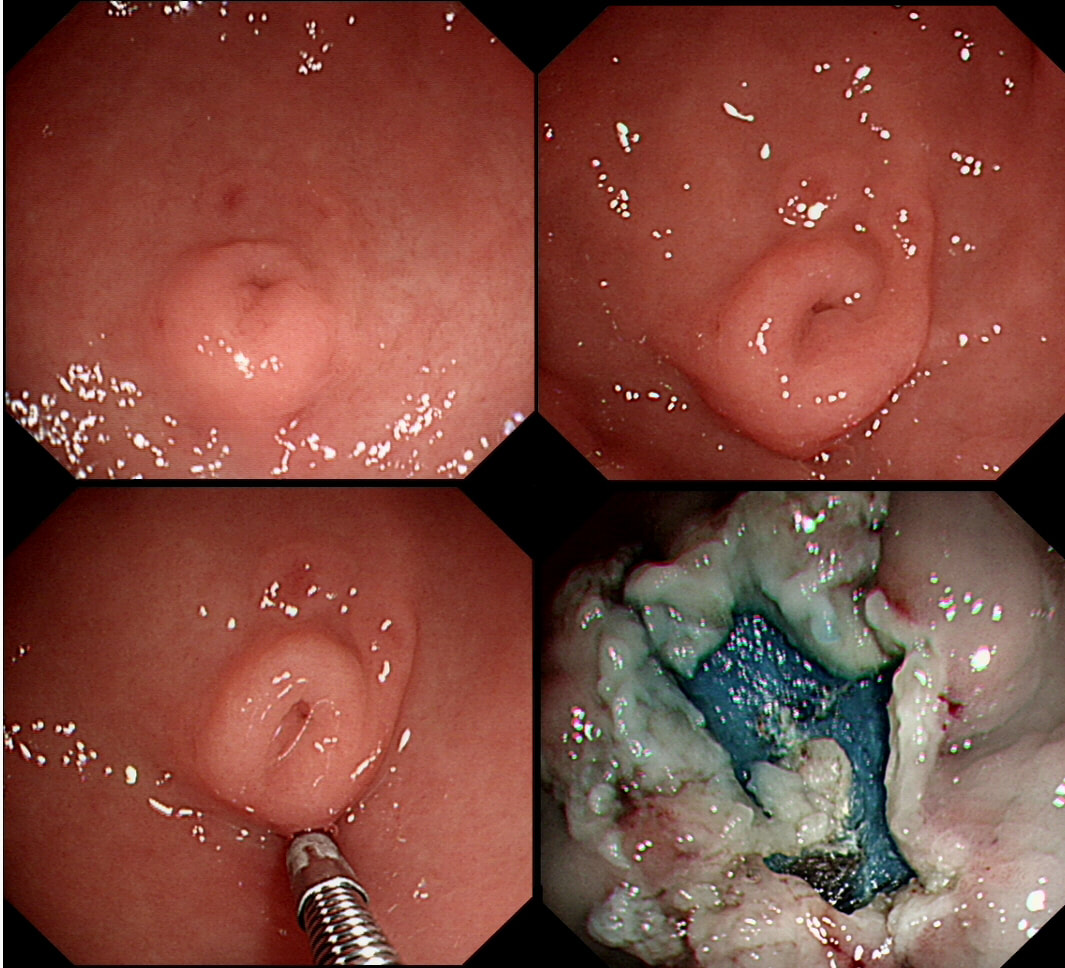
|