
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
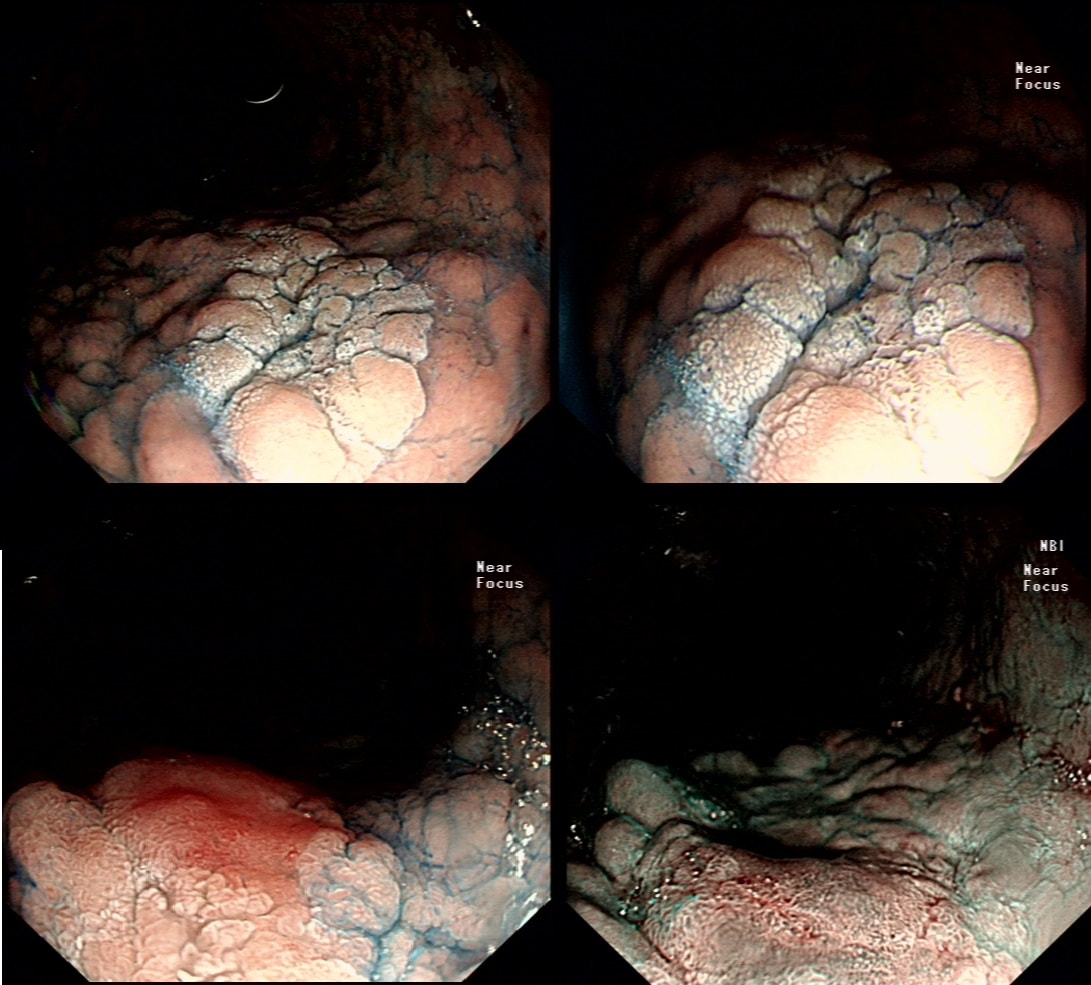
This was polyp found on the greater gastric curve.
WHAT IS THE LIKELY DIAGNOSIS?
explanation
Clearly there is a discrete nodule containing some small round crypt openings. If a dysplastic (mutated and genetically unstable) lesion produces a visible lesion, the pathologist calls it an 'adenoma'. Dysplasia in a flat mucosa is just called 'gastric dysplasia'. Of course in the colon there is a long established 'adenoma → carcinoma' sequence first proposed by Basil Morson a famous British pathologist. He estimated that about 2/3 colorectal cancer must be arising from an adenomatous precursor. What gives rise to the rest remained a disputed mystery until Jeremy Jass, another famous pathologists (and I really nice guy as I found, meeting him at a conference) proposed that serrated polyps may also give rise to cancer [Histopathology 2006;49:121-31]. His suggestion and data to support it, didn't really go anywhere for some 10 years but after he died in 2008 of glioma, the 'serrated pathway' to bowel cancer has become accepted.
Anyway, in the stomach things are even more complicated! There are at least 4 types of adenomas:
Of course, not every gastric polyp is adenomatous. Most are hyperplastic and look angrily red (because they have lots of capillaries) and often with white fibrin caps, making them look a little like mushrooms and may have a villiform surface reminisient of TVA's in the colon. Another common type are the 'Fundic gland polyps' which are full of cystic spaces and therefore look a little like frog-spawn. These usually develop in patients on PPI's but also in FAP. Polyps may also be hamartomatous as in 'Peutz-Jeghers syndrome', 'Cronkhite-Canada syndrome' and 'Juvenile polyposis'. By the way, the word 'Hamartomatous' implies that the polyp has arisen from overgrowth of multiple aberrant cell lineages rather than from a single, mutated precursor cell as in an adenoma. And then of course there are neuroendocrine tumours (NET's). A whole different thing which has a complete podcast dedicated to it. You can tell that a gastric polyp is a likely NET as they usually have little vessels crawling up it's sides. Finally, the lesion may be a gastric metastasis most commonly from breast, kidney, melanoma or HCC. By the way, there is a pitfall here as 'lobular breast cancer' mimics diffuse type gastric cancer. For this reason you should inform the pathologist if the patient has a history of breast cancer and you suspect a metastasis! |