
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
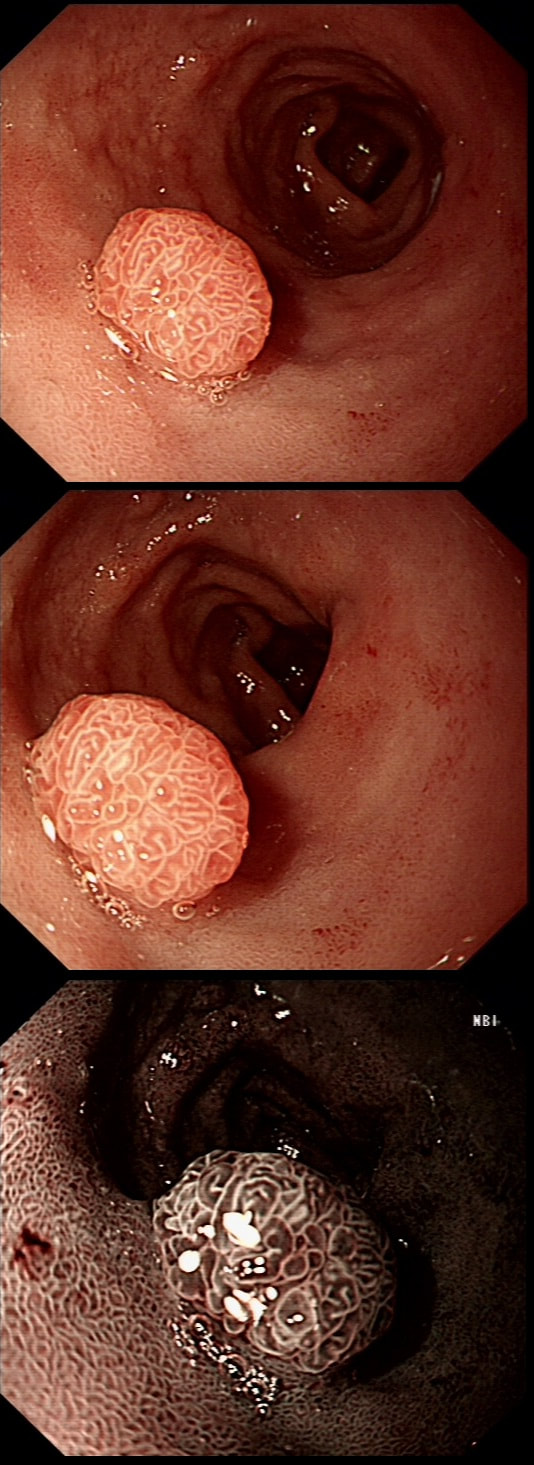
A rather beautiful polyp found in the duodenum of a patient undergoing upper GI surveillance
WHAT IS THE LIKELY HISTOLOGY?
explanation
This polyp doesn't look adenomatous. Remember that in the duodenum, the adenomatous polyp are usually flat, often with white white edges and with a slit-like or gyrate crypt pattern. Of course, in this case the crypt pattern is gyrate, almost exaggerated gyrate! The rather beautiful surface rules out an inflammatory polyp and an NET, both of which don't have this pretty surface structure. Even the histology is rather beautiful, see example below!
In addition, as you probably know, most duodenal NET's will have a central indentation and will not have a distinct crypt pattern. Cutting to the chase, this patient has Peutz-Jeghers syndrome ! This is a good example of the hamartomatous polyps these patients develop throughout their GI tract. Similar hamartomatous polyps also develop in the 'Cronkhite-Canada syndrome and Juvenile polyposis. Hamartomatous polyps are characterized by 'disorganized overgrowth' of the normal tissue but without visible cellular instability (dysplasia). Of course, these patient have an appalling lifetime risk of developing cancer which can be as high as 90%, including gastric, colorectal, breast, colorectal, and pancreatic malignancies. Unfortunately, there is no no evidence that removing hamartomatous polyp will reduce the subsequent risk of cancer. For this reason the only justification for attempting the somewhat hazardous endeavour to remove PJS polyps deep within the small bowel is to reduce the risk of subsequent intussusception. Rather surprisingly, a quick medline search has not revealed any RCT evidence that this actually is worthwhile ! 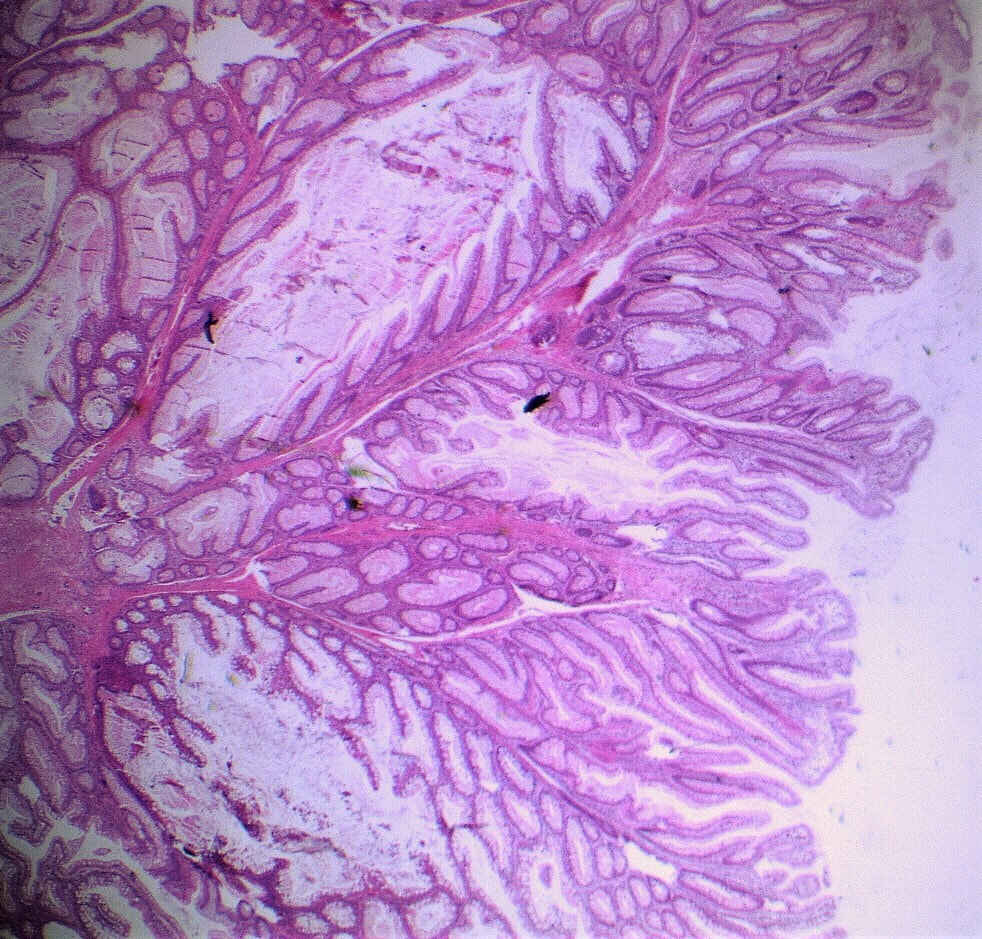
|