|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
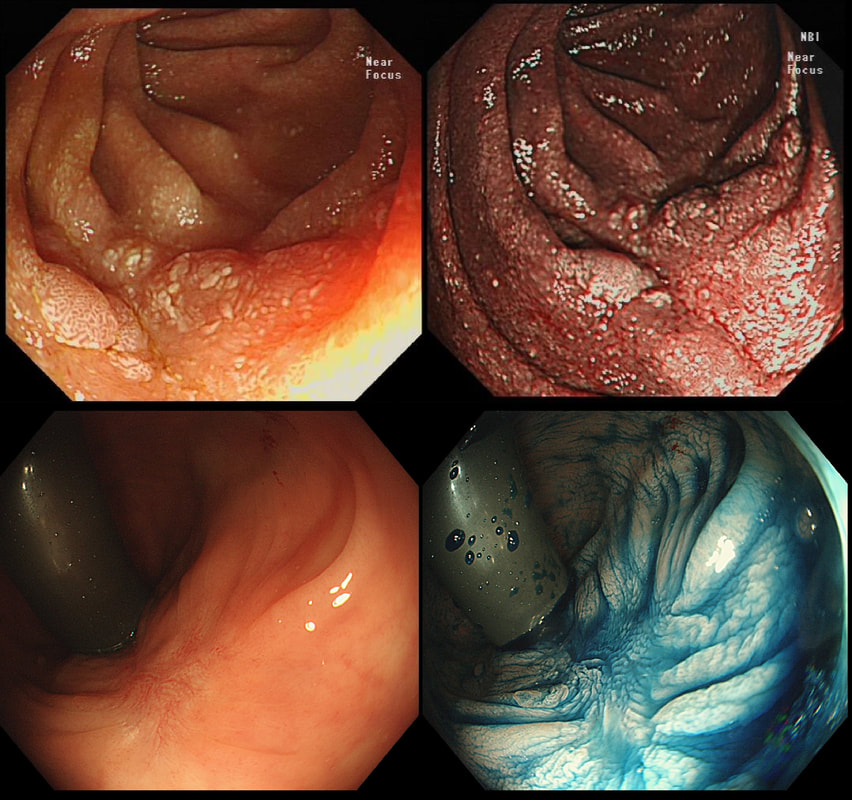
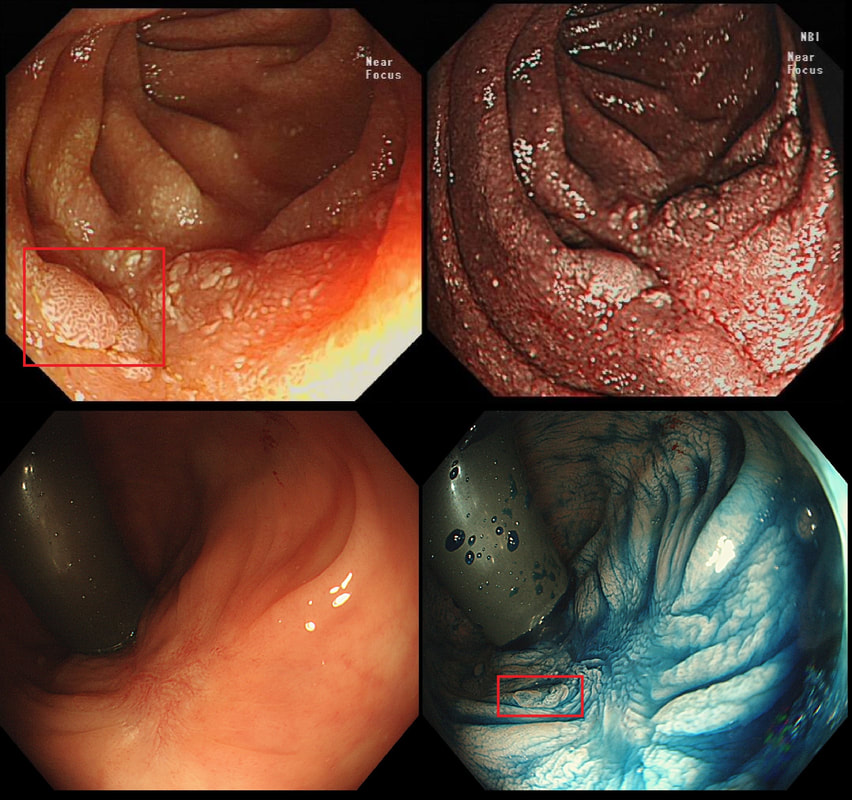
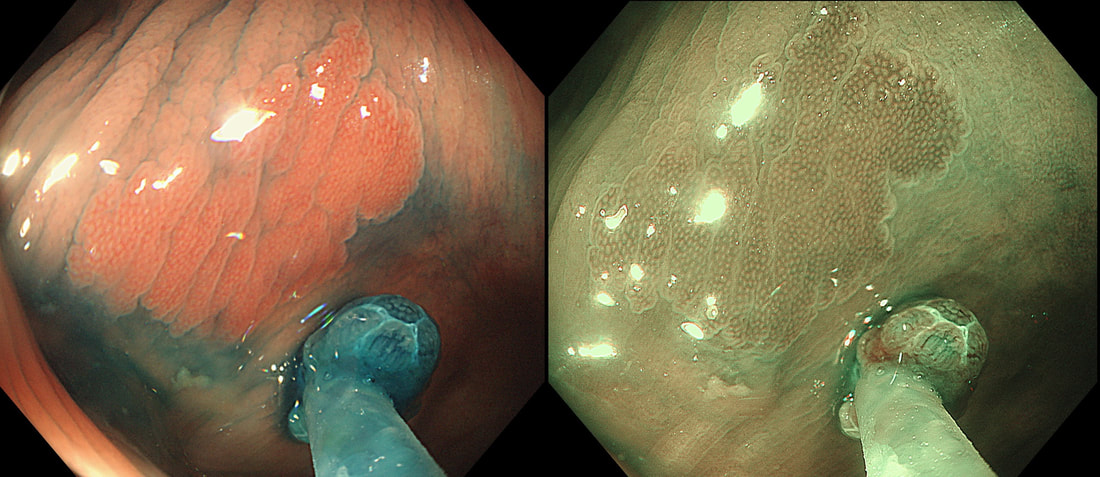
Two EMR sites. The top in the duodenum and the bottom in the rectum
ARE THE SCARS 'CLEAN'?
explanation
The teaching point behind these two images is the simple message that it's impossible to see a local recurrence with just 'white light'. You must assess the scars with NBI or dye sprye or both (I do)! In addition, remember that most local recurrences are to be find at the most 'difficult to see edge'. Perhaps you can only see a local recurrence in retrovertion?
In these particular cases both have a local recurrence (see below).

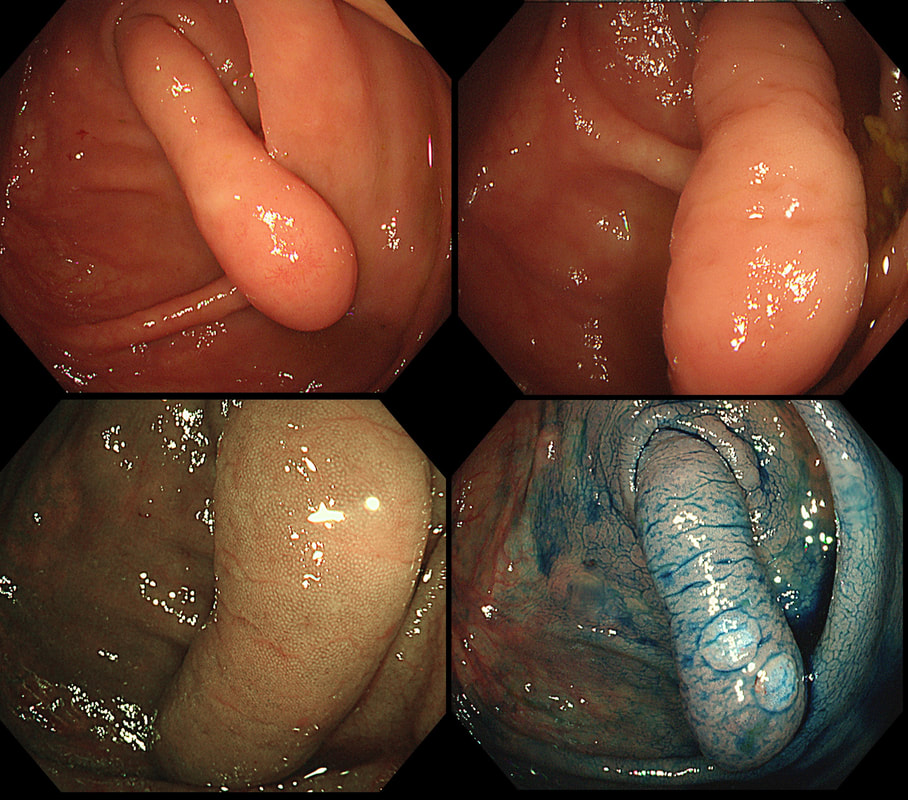
This polyp was found in the caecum.
WHAT'S THE LIKELY DIAGNOSIS?
explanation
I did hesitate for a moment as the lesion did, at first sight seem to arise from the caecal pole and was reminiscient of an inverted appendix (see below). However, on closer scrutiny, it has the typical wide-open crypts of a 'sessile serrated polyp' and wasn't actually that close the the caecal pole. It was removed without incidence after injecting some saline below.
Three colonic polyps to choose between !
WHICH IS THE MOST SUSPICIOUS?
explanation
B has a lovely brain-like crypt pattern of a rather pretty TVA. Of course, C is difficult to assess as the surface crypt pattern may not reflect was is lurking deep inside. Data from the NHS Bowel Cancer Screening Programme (see table below) puts the risk of cancer in a >45 mm at 15%. For this reason, the polyp should be removed in as few fragments as possible.
However, A is the polyp which I think looks most suspicious. It has a suspicious central nodule and on the NBI image (top-right), I don't see an organised crypt pattern in parts of the polyp. This is a superficially invasive cancer which was just invading into the muscular mucosa (sm1 invasion)! it lifted well enough for a resection. Again single fragment resection would be paramount when removing this polyp. Below is a table which I received from Matt Rutter a few years ago. It links size with histology for polyps resected on the NHS Bowel Cancer Screening Programme 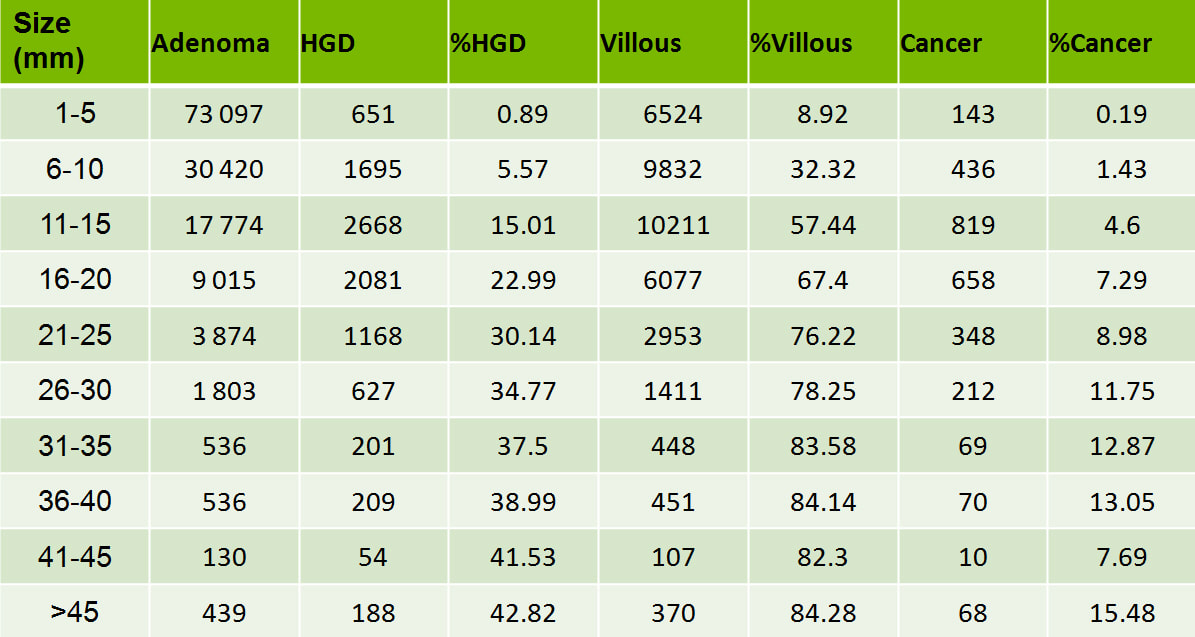
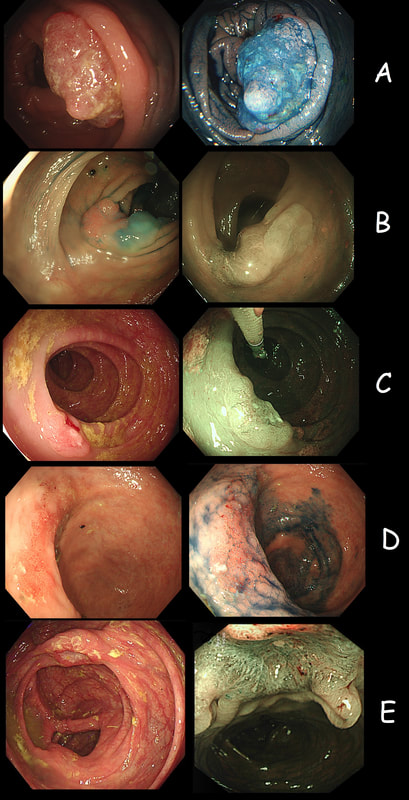
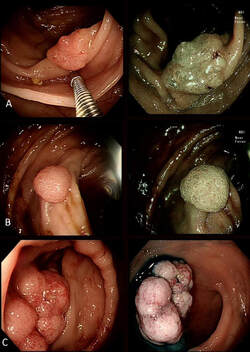
As you know, colonoscopy protects less well against future cancer in the right hemi-colon, than cancer elsewhere in the colorectum. Here are 5 lesions, all found in AC. Four are malignant and one isn't ...
WHICH ONE IS NOT A CANCER?
explanation
You can probably tell that the first lesion is a cancer because of it's nobbly surface and lack of crypt pattern in places. It was a sm1 invasion T1,N0 cancer (i.e. invading up to the muscularis propria layer but didn't invade into it).
The second lesion is a sessile serrated lesion with a small cancer at it's edge. The staging was identical to the first lesion (sm1 invasion T1,N0 cancer). The third lesion was a superficial carcinoma (sm1 invasion only) and the only in the series actually removed endoscopically. The fourth lesion is the 'odd one out'. It's actually a 'caecal patch' in a patient with ulcerative colitis, only affecting the rectum. The final lesion was a 'mucinous adenocarcinoma'. Interestingly, analysis of the initial biopsies reported 'TA+LGD'. Don't believe everything those pathologists tell you! Your eyes don't lie! There is a further interesting twist here. After another set of samples, got the pathologists to agree with our endoscopic diagnosis, we were surprised that the patient was turned down for surgery due to severe comorbidities. Rather begs the question what was the point in putting the 85 year old gentleman through two colonoscopies !!! Anyway, that was 4 years ago and he has still not developed any symptoms from his cancer!? A recent CT confirmed that it was slowly growing and was now annular but without any evidence of spread or obstruction. Interesting and clearly turning someone down for surgery is not necessarily a 'bad thing' ! Still leaves me wondering why they keep scanning the poor bloke though? Below I've attached a reminder about the 'Kikuchi staging' which your pathologists should use to stage superficial flat cancers. 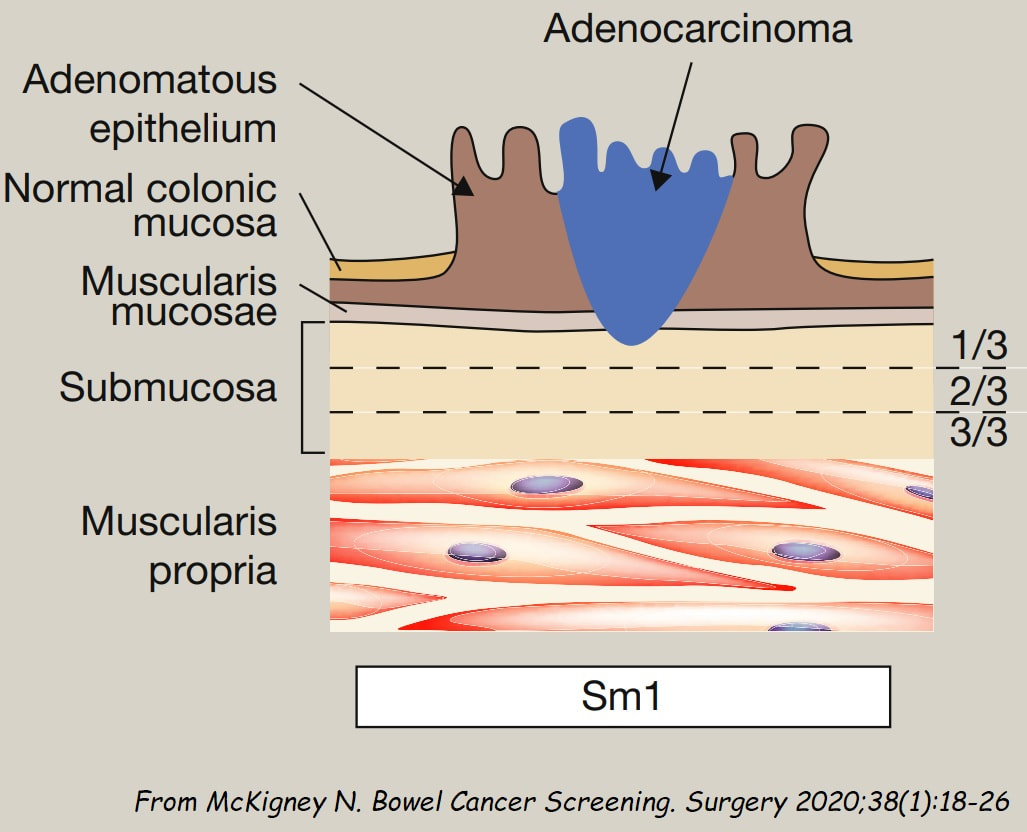
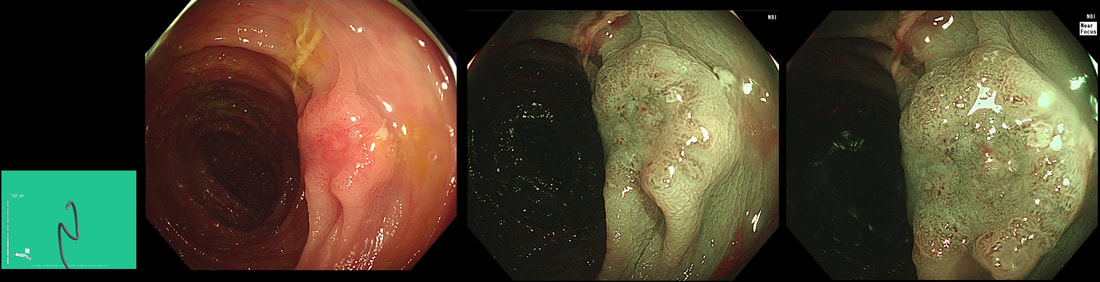
This 13mm colonic lesion has been referred for resection
WHAT IS YOUR PREDICTED HISTOLOGY?
explanation
Histology had 'informed us' that this was a TA+HGD. But of course, Endoscopically this IS A CANCER! 'Newbies to endoscopy' may wonder how I can be sure?
Simply, this is what early colorectal cancer looks like !!! Of course, some cancers are hidden deep within larger, sessile or pedunculated polyp and can not be glimpsed from any disturbance of the polyp surface. That is a separate issue and no amount of experience can help you with the chance finding of cancer buried deep within such a polyp. Attempting to find the words to describe the features which are 'malignant' is difficult. Firstly the lesion is firm! If you can reach it with a finger, you will find that it's hard to the touch. If you can poke it with the biopsy forceps you will find that it moves like a solid disc of firm tissue. It's also the elevated margin surrounding an angrily red centre which has a different crypt pattern is another feature. Actually, there does appear to be some sort of crypt pattern in the centre. Endoscopically we had diagnosed sm1 invasion (i.e. invading into the top 1mm of the submucosal layer). Surprisingly, it didn't lift at all and because the patient was not a surgical candidate, we offered a 'full thickness resection' (images below). Rather surprisingly, the final diagnosis was of sm3 invasion with LVI! With time you will find that removing cancers endoscopically never leaves you with absolute 'peace of mind'. There is always some adverse feature to keep you awake at night! 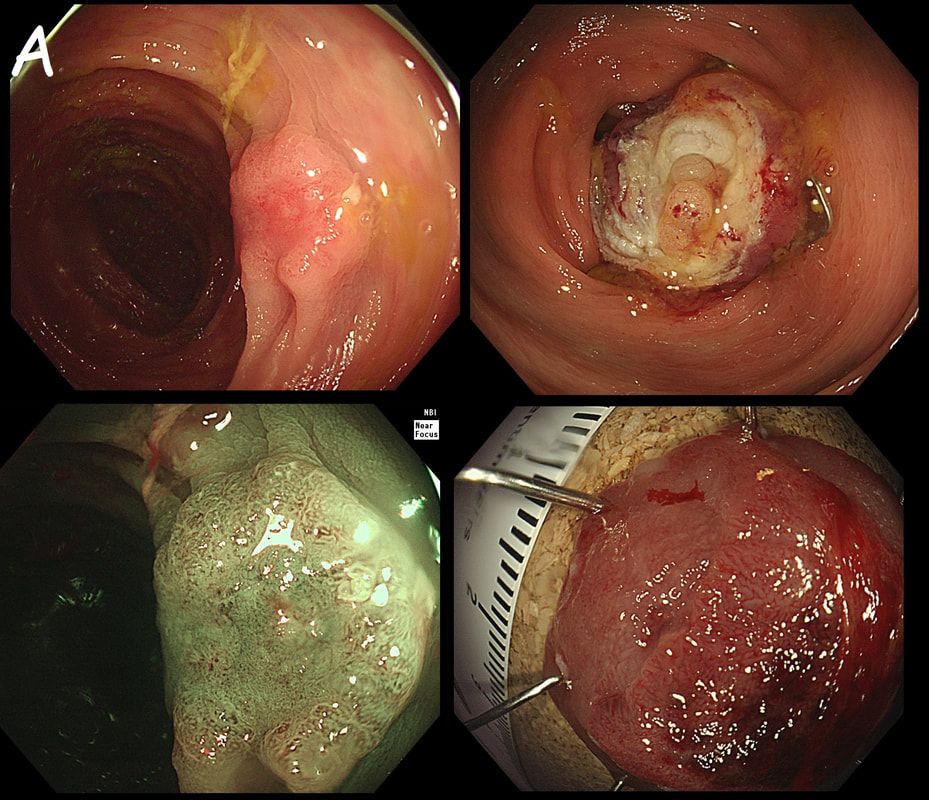
This patient has undergone a right hemicolectomy for cancer some 2 years earlier. He now attends for his first "post - surgery" colonic surveillance examination. This was found at the anastomosis.
WHAT IS YOUR DIAGNOSIS?
explanation
There is no discernible crypt pattern, not because of cancer, but because these polyps are composed purely of granulation tissue! I also thought that it looked a little odd and took some samples (which I don't usually do when my endoscopic diagnosis is of "granulation tissue" at an anastomosis). Here is another example of granulation tissue, this time at a colonic EMR site, which looks worrying to the unwary ☺!
A beautiful polyp removed from the ascending colon. WHAT IS THE LIKELY DIAGNOSIS? explanation
This is a typical inflammatory polyp! The pathologists call these inflammatory/hyperplastic polyps. However, for clarity I wish that they would simply call them 'inflammatory polyps'. After all, pure 'hyperplastic polyps' are actually a different entity in the colon consisting of mutated epithelium. In contrast, 'inflammatory polyps' like this one consists of granulation tissue! As you probably know, the white spots are superficial caps of fibrinopurulent ulcer slough overlying small spots of ulceration. It remains a mystery why such a spectacular lump of granulation tissue developed in this particular patient. There was no history of NSAID use but the patient did have 'neurofibromatosis' and the lesion was found at a surveillance examination. This polyp was found in the transverse colon. It has not previously been sampled! WHAT IS THE LIKELY HISTOLOGY? explanation
This is a rather interesting polyp. Well its starts off looking rather booring but after the submucosal injection it changes. Rather than a bland looking TA, it appears to be somewhat tethered in it's centre. I suspect that the subtle central dip would have been evident on retroflexion but retroflexion in the ascending proved impossible. Just look at how the scopeguide shows the shaft keeps buckling in the sigmoid and transverse, in spite of abdominal pressure to try to limit its movement. With suboptimal lift, you of course have three options: ESD, piecemeal EMR or choosing a more powerful, superstiff (but more dangerous) snare. I opted for the latter option (I usually do) and with some difficulty managed to capture the polyp single fragment. Arguably, as this lesion is a 'LST-D' type of lesion a piecemeal resection may have been less appropriate. The LST-D's are usually either HGD/IMca or superficially invasive cancer. The lift is good, telling you that it's not an invasive cancer after all. . On the other hand, a single fragment ESD may be linked with a 1:20 risk of a microperforation. In all honesty, probably not any different to the risk of perforation with a superstiff snare! 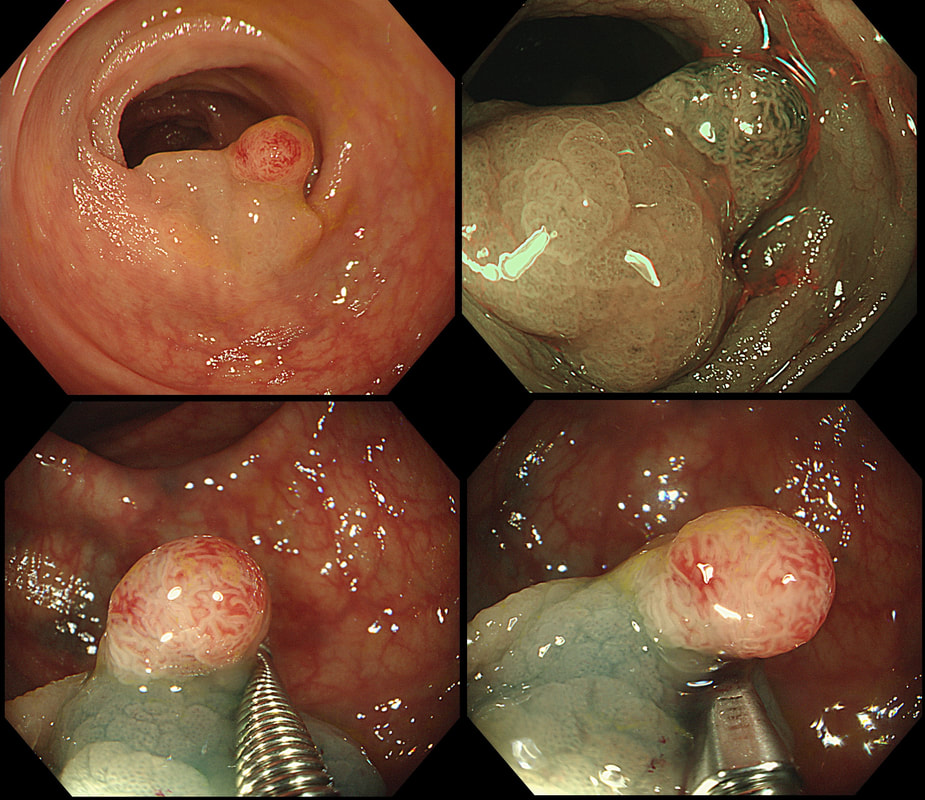
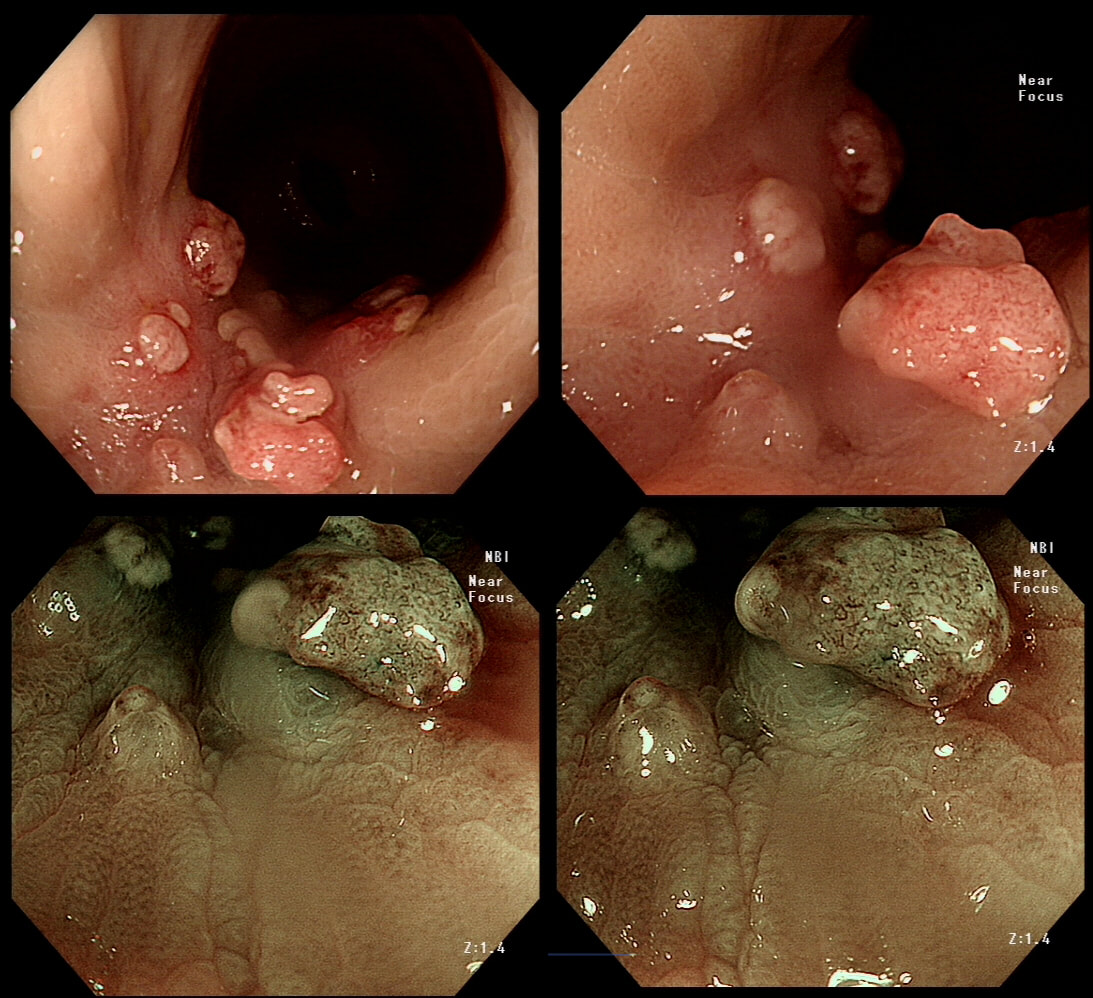
This polyp was found in a 30 year old patient with a family history of bowel cancer undergoing colonic surveillance because of a 'polyp syndrome'.
WHAT IS THE LIKELY POLYP SYNDROME?
explanation
This proved to be a difficult question and only 15% of our facebook group got the correct answer of: Serrated Polyposis Syndrome !!!
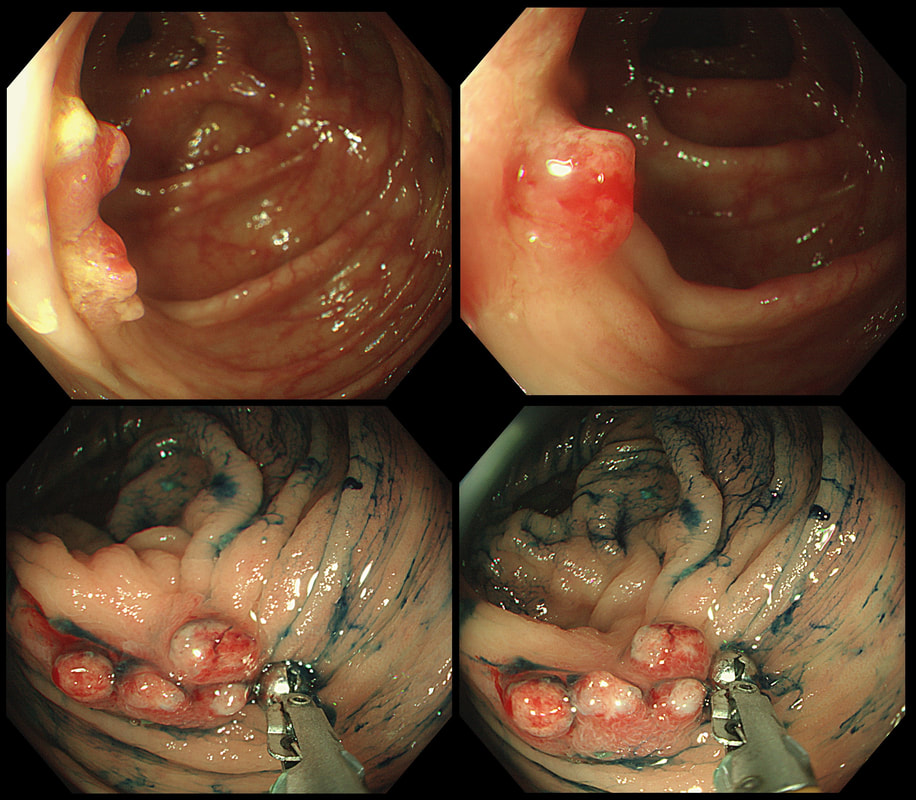
The odd thing about this polyp is that it appears to be a tubular adenoma (slit-like crypts) arising from a broad somewhat odd looking fold. The 'fold' is actually a larger hyperplastic polyp. Of course large hyperplastic polyps are now referred to as 'sessile serrated lesions' (SSL's). You are looking at an SSL, sprouting a TA !? A 'purist' histopathologist may refer to this entity as a 'mixed serrated, adenomatous polyp'. Do you know of a polyp syndrome where patients have a mixture of SSL's and adenomatous polyps? Of course, the serrated polyposis syndrome 'SPS' (previously called the sessile serrated polyposis syndrome). It's now realised that many patients with serrated polyposis syndrome actually have a mixture of serrated and adenomatous polyps. It's possible that these patients have a greater risk of developing cancer. The correct answer is therefore 'A' ! The BSG has published a 'position statement' on the topic of SSL's which is well worth reading. The BSG sensibly recommend annual surveillance until all serrated polyps above 5mm have been cleared, following which the surveillance interval may be reduced. This is because patients with SPS do not seem to have a higher risk of developing cancer than patients with Lynch syndrome. 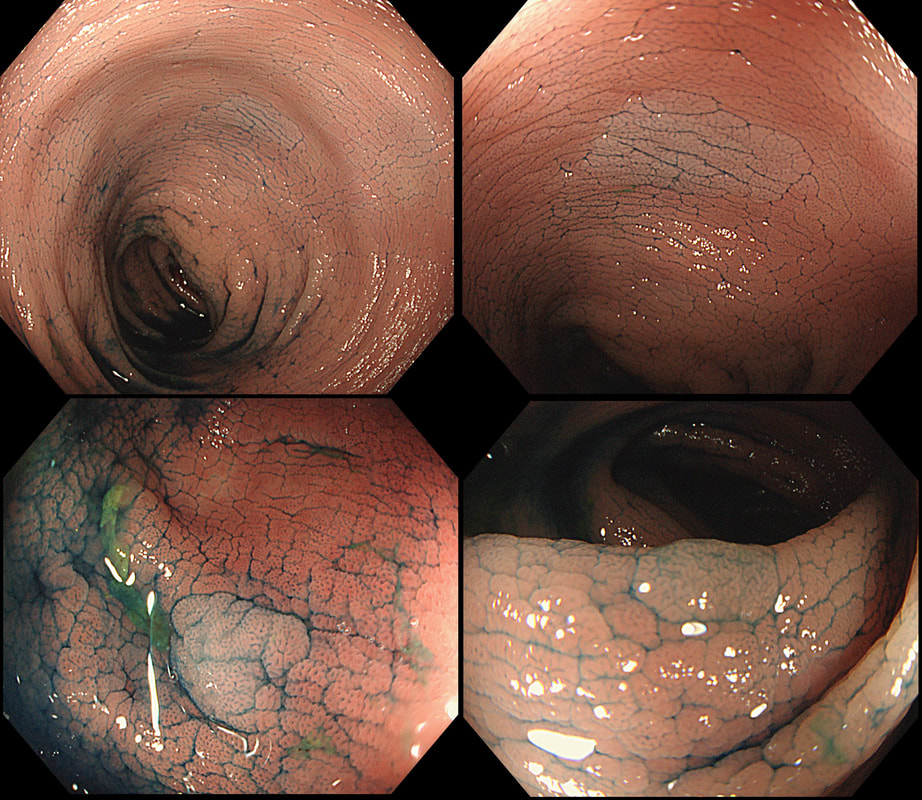 This is the colon of a patient with long-standing colitis and PSC on annual surveillance. These were found after indigo carmine dye spray. WHAT IS YOUR ENDOSCOPIC DIAGNOSIS? a) patches of crypt distortion b) serrated lesions c) a flat adenomas Explanation
Actually, these are patches of 'crypt distortion'. Often seen after pan-colonic dye spray and VERY difficult to distinguish from serrated lesions. The crypt openings are a little larger than normal and strangely these seem to develop in patches which can be very large. In a case like this, I would take samples to reassure and alert subsequent surveillance colonoscopists to the presence of these odd lesions. In my experience they are usually seen in long standing colitis which has been troublesome in the past and I wouldn't be entirely surprised if future research find that these are more commonly found in patients who go on and develop flat dysplasia in the future. Below is a close-up of a lesion.
|