
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
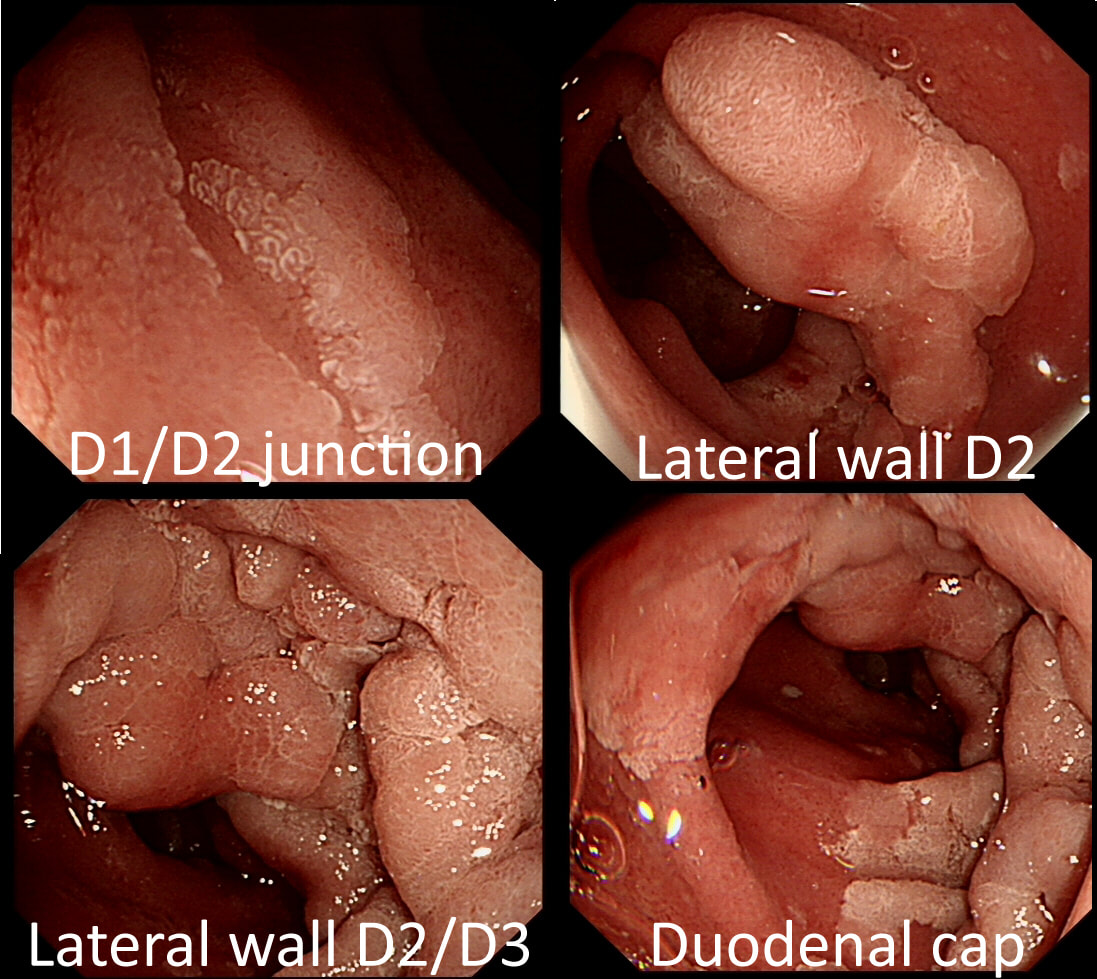
A fit middled aged patient with FAP is referred for consideration of a duodenal EMR for his duodenal polyposis. Earlier samples have indicated that this is a villous adenoma harbouring up to high-grade dysplasia (VA+HGD).
SHOULD WE ABORT OR ATTACK?
explanation
The Spigelman score is a little peculiar in that patients with scores of 0 to 3 have a very low risk of developing cancer. However, when patients accumulate a score of 4, surgery should be considered as there is a high risk of cancer.
Of course, many patients with FAP have desmoids which precludes surgery. In those cases I consider intervening endoscopically if: 1) the patient is fit enough to survive emergency surgery to sort out a perforation or cope with a 4+ unit blood loss AND/OR 2) there is a higher than average risk of cancer, for example in a patient with extensive HGD or confirmed IMca. Of course, the lesion also has to be 'resectable' within your level of expertise. Personally, I find lesions situated at 12 O'clock the most challenging to remove. Furthermore, a general anaesthetic is probably a prerequisite for resections taking longer than 20 min or so (which they always seem to do). Thus, I consider the "correct" answer to be 'Abort'! I decided that the lesion was likely to be too large for me to resect. Fortunately, the patient was a good surgical candidate. A 'pancreas sparing duodenectomy' was carried out and a TVA with mainly LGD but also areas with HGD was completely removed. Postoperatively the patient developed pancreatitis and was discharged 4 months later... Clearly this is 'Tiger Country' for surgeons as well ! |