
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
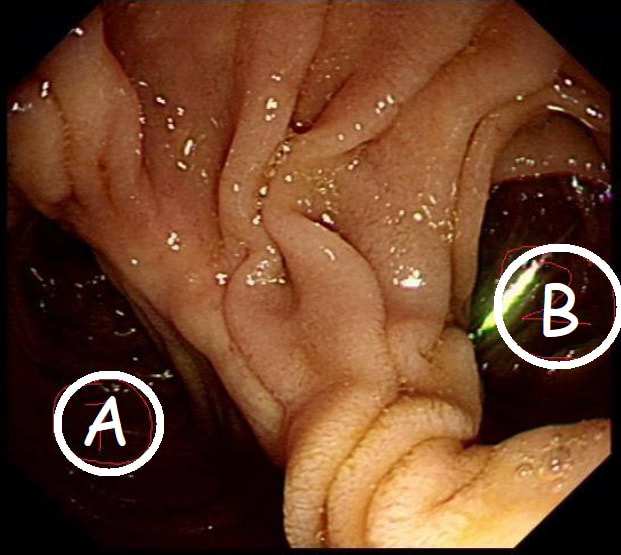
This is the gastric anastomosis of a patient who has previous undergone a Bilroth II distal gastrectomy.
WHICH PATH IS MOST LIKELY TO LEAD TO THE AMPULLA?
explanation
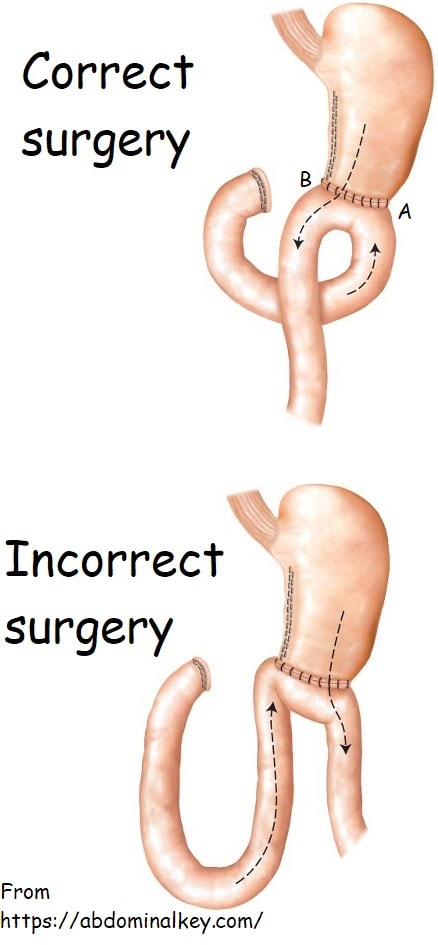
At a 'correct' Bilroth II operation, the 'afferent limb' (taking bile to the stomach) should be placed on the greater curve (path A in the photo) and the efferent limb (taking food away from the stomach) should be on the lesser curve (path B). The reason why surgeons don't to it the other way around is that kinking and obstruction is then more common.
It's something of a trick question as at Enteroscopy, you would aim to get down the efferent limb (B). However, if your aim is to reach the duodenal ampulla, you should choose route A ! Dr Yano proposed a trick was [Yano T. Endoscopy 2012;44:E340-1] to help you at Enteroscopy. You inflate the 'distal balloon' (assuming that you are using a double balloon enteroscope of course), and instil 50 mL of indigo carmine solution beyond the tip of the scope. Peristalsis will not favour the afferent limb and the afferent limb will have less indigo carmine dye. Even when you get to the distal 'Y' in the Roux-en-Y', it will also help you (see below). The accuracy of this method is said to be 80%. However, I've come up with an alternative method! Give your patient a cup of 50ml of dilute indigo carmine dye to drink some 30 minutes before your examination. Of course you must warn him that the urine will be blue/green for the rest of the day. If all goes to plan, at Enteroscopy you will find that "the route which is blue is the way to go" ☺ ! 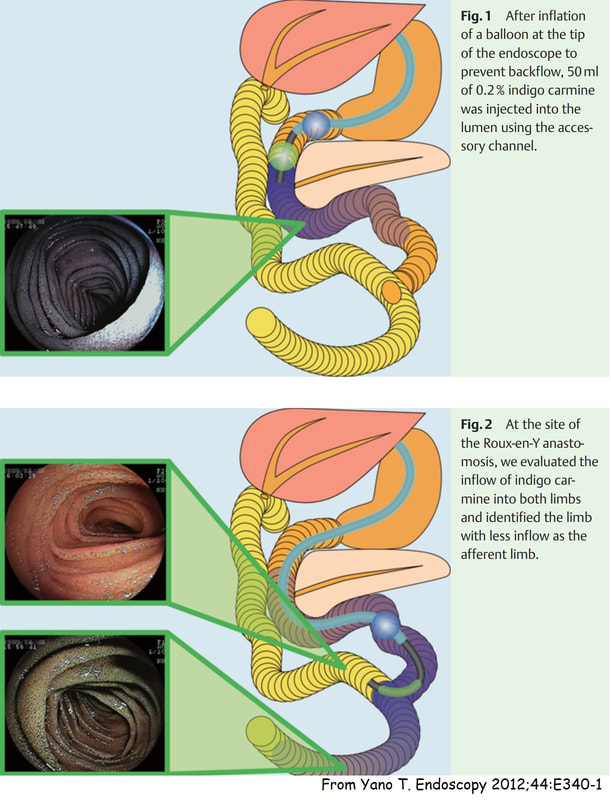
|