
|
|
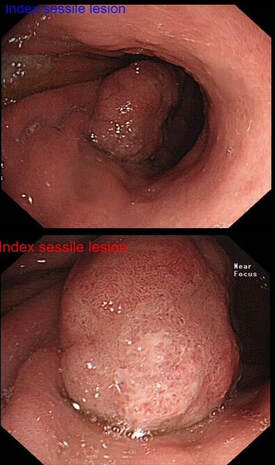 Of course, its important to carefully examine the entire stomach especially in premalignant stomach for any synchronous lesions despite seeing something very evident. The above video is follow up Endoscopy 3 months after the removal of the large sessile lesion in the antrum (photo). The polyp was removed by ESD and histology confirmed a Villous adenoma with low and high grade dysplasia as well as a small focus of adenocarcinoma – pT1aM2 (clear margins). Wisely, it turned out, the patient was recalled for early 'site-check' and examination of the rest of the stomach. This turned out to be worth while ! WHAT DO YOU THINK THE LESION IN THE VIDEO IS? explanation
It is very easy to overlook synchronous lesions when there is a large 'eye-catching' lesion, drawing all your attention. My learning point is that its important to look for synchronous and eventually metachronous lesions and not to get blinkered by the obvious pathology! Patients do sometimes have dual pathology ! Yes, it happens !!! Actually, the second lesion was confirmed to be an Intramucosal adenocarcinoma - moderately differentiated pT1aM3, with no lymphovascular invasion and clear lateral and deep resection margins . This was a 'curative resection' as per BSG Guidelines for endoscopic resection as the risk of nodal metastasis in such leisons is probably <1%. Some bullet points on Synchronous tumours (Dysplasia or cancer)
And some on the topic of Metachronous tumours
Reference Banks M, Graham D, Jansen M, et al British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut 2019;68:1545-1575. |