|
This study from Nottingham provides an introduction to the 'Vienna classification' and an illustration of how difficult it is for histopathologists to be equivocal on low grade dysplasia versus innocent 'atypia'. After all, there is no 'stain' for dysplasia which can be used to decide on the matter. But all is not lost! By asking several pathologists to give an opinion and by requesting p53 immunohistochemistry, you can get closer to the truth ! Kaye PV. Barrett's dysplasia and the Vienna classification. Histopathology 2009;54;699-712 |
|
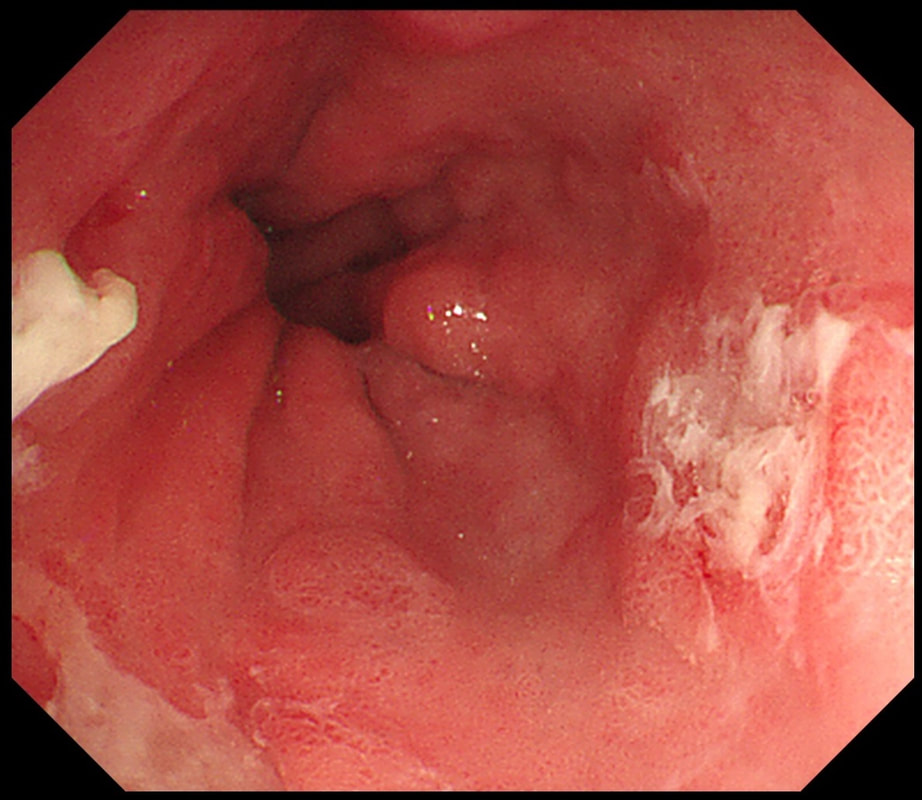
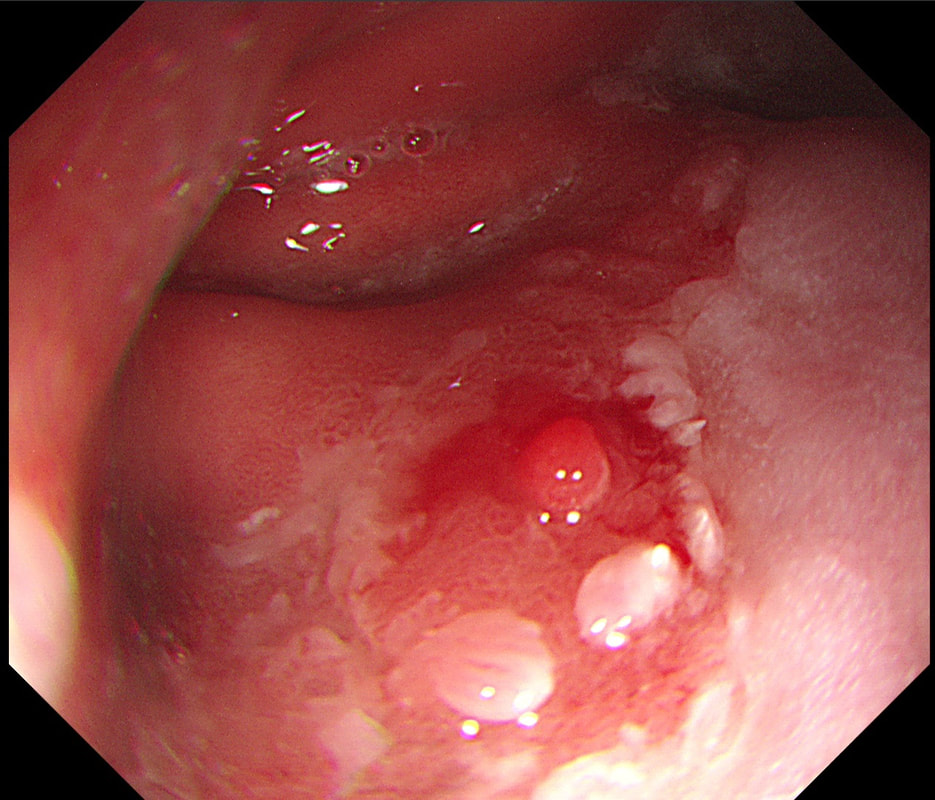
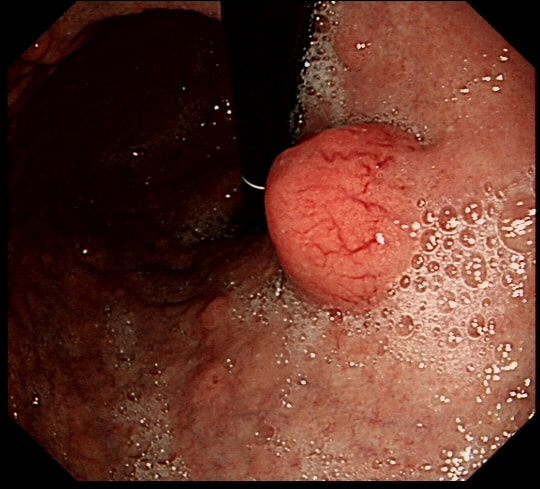
The endoscopic assessment of Barrett's is notoriously difficult. My own simple rules of thumb are: 1) all nodularity is evil and 2) all ulceration is evil. However, if you want to take things further, this article from Nottingham is a good place to start! Singh R. NBI and magnification in Barrett's. Endoscopy 2008;40(6);457-63 |
|
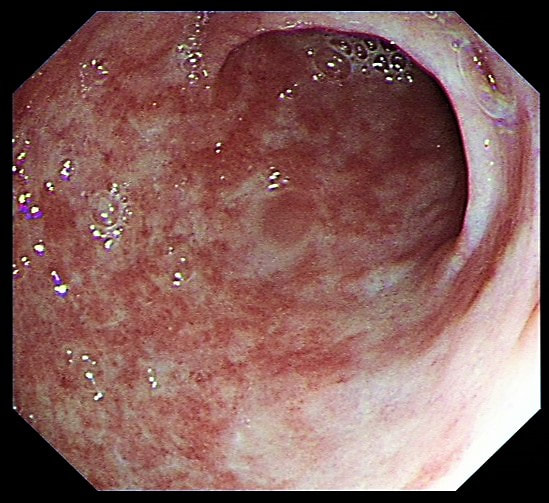
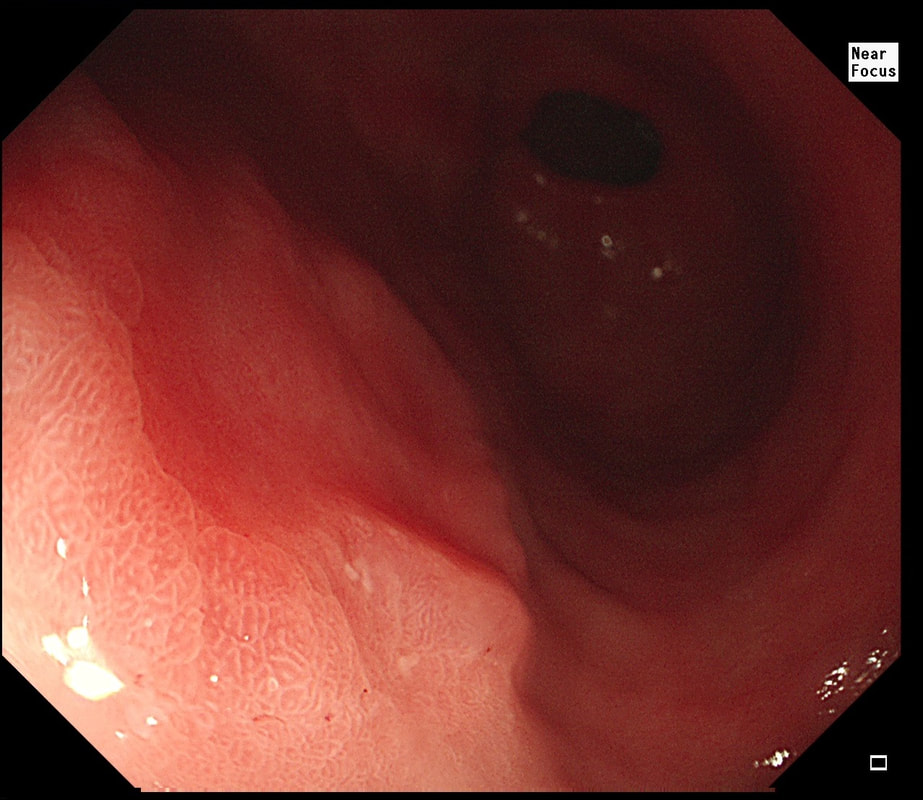
The upper GI tract is easier to get around but far more difficult to assess for Endoscopists. There is a lot of subtle pathology which is easy to miss! Arguably the first thing to learn is to recognise Hp associated chronic gastritis and then to look further for gastric dysplasia and early cancer. This review for China is an excellent overview. Even the impenetrable Kimura-Takemoto classification makes sense! Soma N. Endoscopic differentiation of HP gastritis vs EGC's. J Dig Dis 2016;17;641-51 |
|
I must admit that I love to use indigocarmine dye spray to find subtle EGC's in the atrophic stomach. However, if you'd rather rely on NBI and magnification, Kenshi Yao tells you what to look for. You will have to be able to assess the microvascular and crypt pattern within the demarcated contours of subtle lesions. Yao K. Magnifying endoscopy for EGC. Endoscopy 2009;41;462-7 |
|
Few issues are as thorny as gastric NET's. They are easy to spot but treacherous to manage. Mark Pritchard gives us a systematic review of the heterogenous studies conducted in this heterogenous topic. His final statement sums things up: 'Due to the complexity of the area, a multidisciplinary management approach is strongly recommended' No shit ! Exarchou K. Management of gastric NET's. APT 2020;51(12);1247-67 |