
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
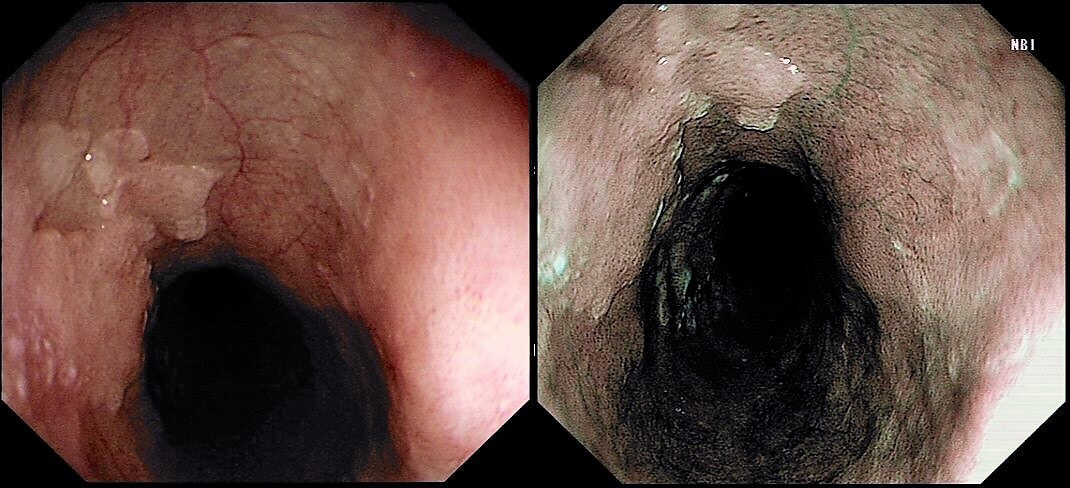
This was found in the distal oesophagus of a patient with dyspepsia. You take some samples.
WHAT WILL YOU TELL THE PATIENT?
explanation
This may be a good example of 'we don't see' because we don't know what it is. Intuitively, we all blank this because it's a benign finding. But what is it? It's actually a patch of squamous hyperkeratosis with some underlying basal cell hyperplasia. The normal squamous basal cell layer is 1-4 cells thick but, in reflux oesophagitis thic increase up to 75% of the epithelial thickness. However, many cases of reflux oesophagitis does not exhibit basal cell hyperplasia and conversely, there are cases which will not be due to reflux disease as in this case!
In rodents (!), the finding has been linked with vitamin deficiencies and zinc deficiency. Of course, squamous hyperkeratosis in the mouth is associated with squamous neoplasia [ J Clin Pathol 2005;58:1325–1327 ] and for this reason, I always take some samples. However, I am yet to find a single case of dysplasia within a patch of oesophageal squamous hyperkeratosis !!! 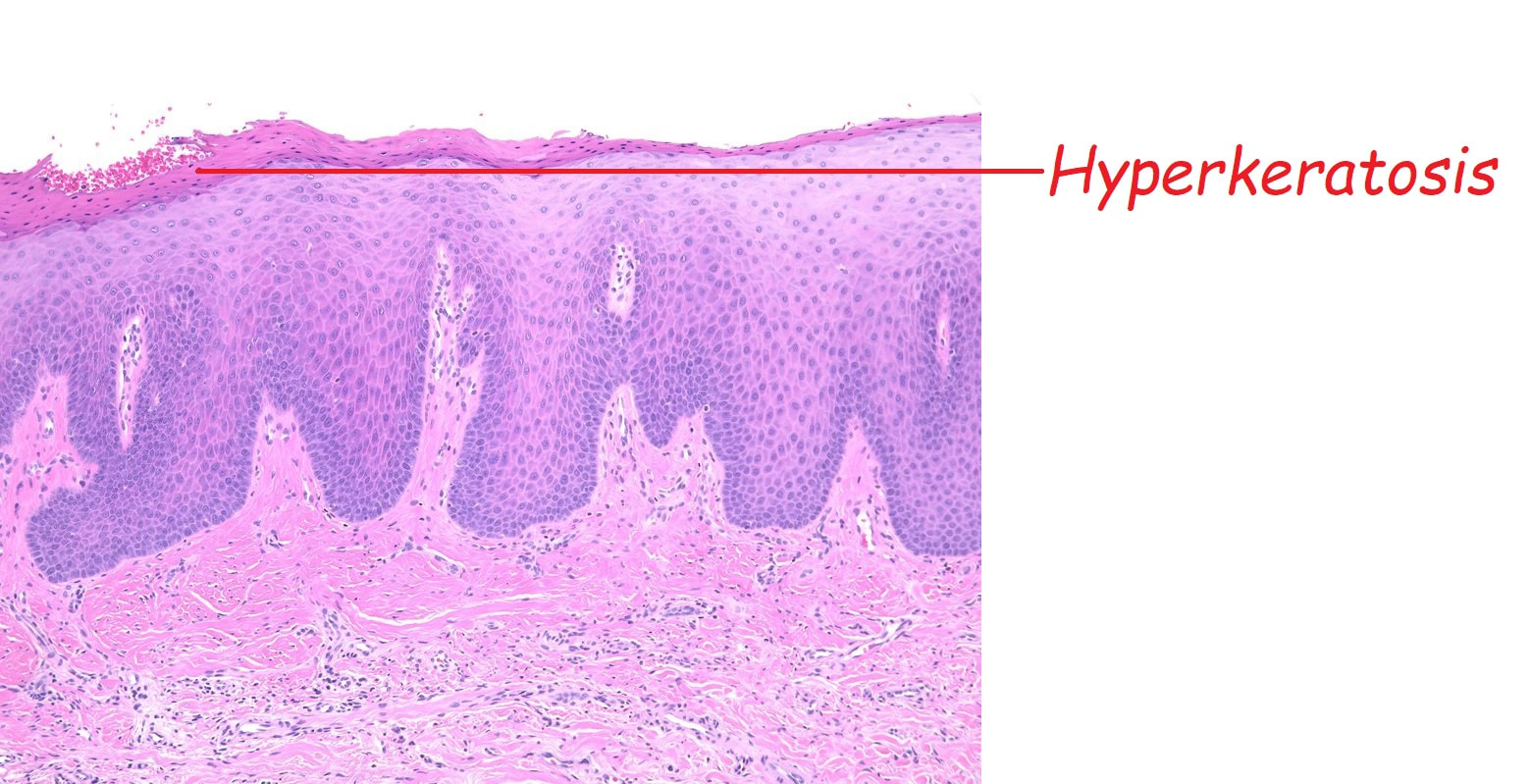
|