
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
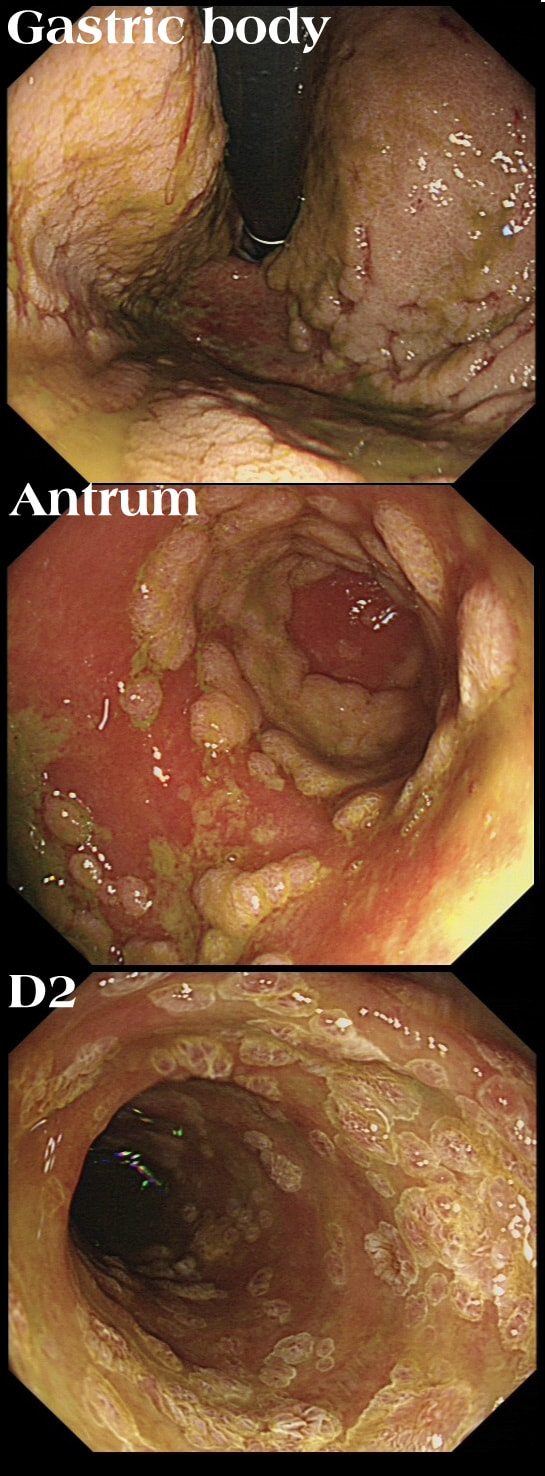
This patient has recently undergone a bone marrow transplant when she develops abdominal pain. PPI therapy has not improved her symptoms and she referred for a Gastroscopy
WHAT IS YOUR ENDOSCOPIC DIAGNOSIS?
explanation
Well this is a striking appearance! I'd never seen anything like it and tentatively suggested HSV gastritis on the histology request form. I didn't consider CMV because there was no mucosal ulceration.
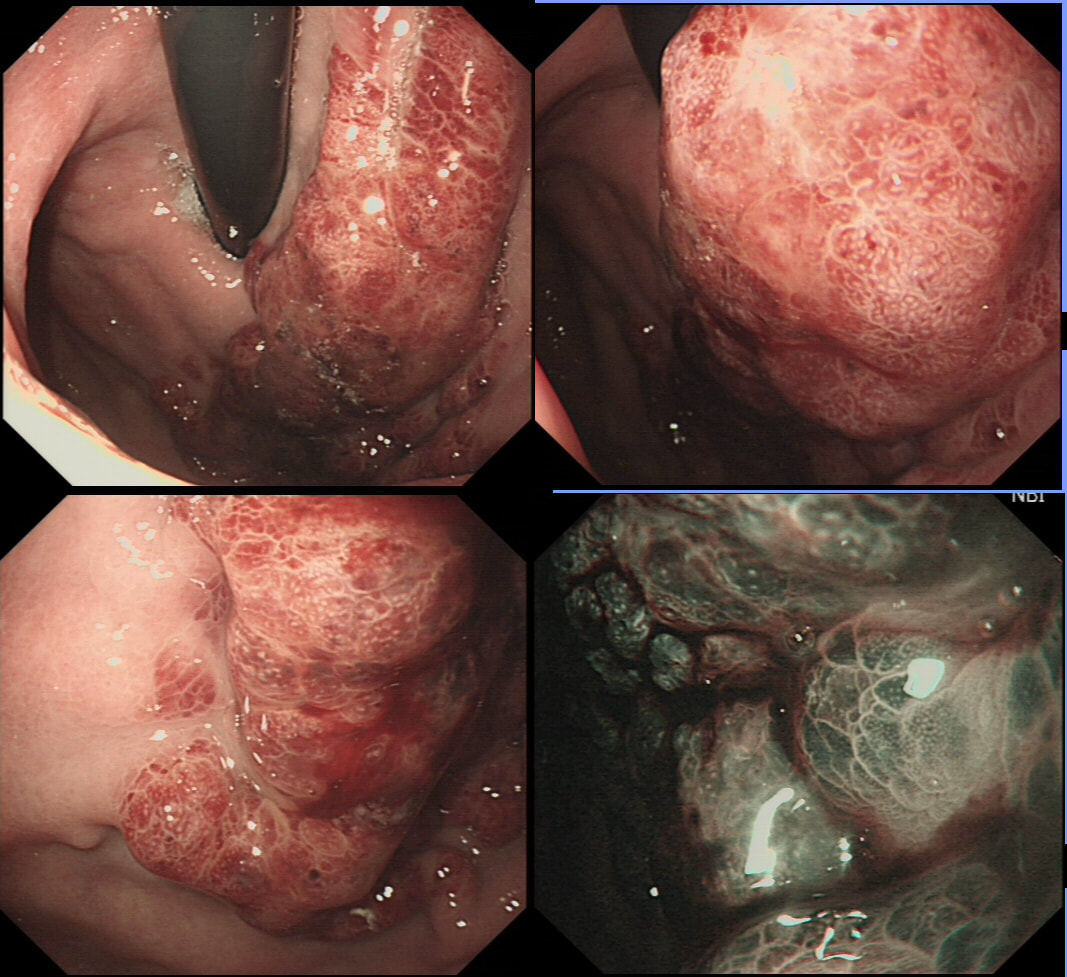
Histology confirmed finding lots of oedematous CMV infected cells with granulation tissue and there was no need for immunostaining for cytomegalovirus proteins. This is a case of CMV gastritis! Actually, there were also some features suggestive of acute GVHD and I can therefore not be entirely sure that these 'plaque-like appearance on the mucosa isn't due to the combined effect of CMV+GVHD+PPI! It's not uncommon, one study, reported that approximately one-quarter of patients who were unresponsive to first-line acute GVHD treatment, actually had coinfection with CMV [Bone Marrow Transplant. 47, 694–699]. Of course, immunosuppressants is the trigger for CMV reactivation but CMV gastritis can occur in apparently immunocompetent patients, although a link with occult cancer has been suggested [Scand J Gastroenterol 2011;46:1228–35]. My guess of HSV was of course unlikely as HSV infects squamous mucosa or the colon (surprisingly), not the stomach. In the oesophagus you may see vesicles and/or small ulcers (left when the vesicles rupture). If I had seen this appearance in the colon I would have called this 'pseudomembranous colitis but of course C.diff doesn't affect the stomach. Can you get gastritis with checkpoint inhibitors? Yes, you can! It can cause a severe, haemorrhagic gastritis as outlined in this article [Case Rep Oncol 2018;11(2):549–556]. There is more information on CMV gastritis at this site. This is the sigmoid colon and rectum of a young patient who have just undergone bone marrow transplantation. WHAT IS THE LIKELY DIAGNOSIS? explanation
In GVHD there are minimal mucosal changes whilst there is extensive ulceration in this case. You do get nasty mucosal ulceration with checkpoint inhibitors but these drugs would not be used in transplantation. C.diff doesnt' cause mucosal ulceration and the herpes virus does not infect columnar mucosa. This leaves CMV ! Cytomegalovirus is a herpes virus that infects the majority of humans. Primary infection in individuals with normal immune function is usually asymptomatic or result in mononucleosis-like syndrome (fever, lymphadenopathy, and atypical lymphocytosis on a blood film). After primary infection, CMV becomes latent in various host cells but are controlled by a functioning immune system. When re-activation occurs in patients with severely compromised immune function (transplant patients or patients with AIDS and CD4 count <50 cells/microlitre), uncontrolled CMV replication can ensue leading to fever, bone marrow suppression, and tissue-invasive disease, depending on where the reactivated cells are residing. Investigations includes serology, pp65 antigenaemia test, histopatholical analysis of any tissue obtained, and PCR based detection. Treatment of choice is oral valganciclovir or intravenous ganciclovir whilst IV foscarnet and cidofovir are second line agents. 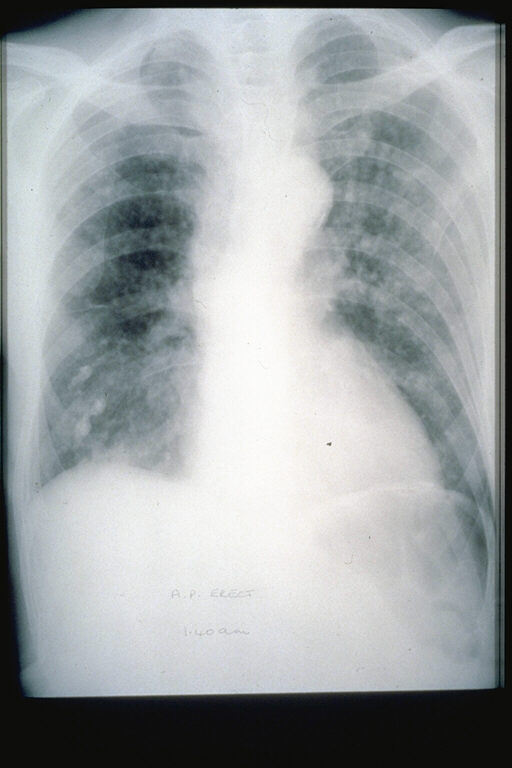
This odd looking thing was found in the gastric fundus of a middle age lady undergoing investigations for nights sweats, a dry cough and shortness of breath on exertion as well as weight loss (CXR enclosed).
WHAT IS THE LIKELY DIAGNOSIS?
EXPLANATION
The patient had a two month history of night sweats, malaise, weight loss. More recently she developed a non-productive cough and shortness of breath on exertion. The CXR shows some diffuse interstitial infiltrates.
Of course, the patient has AIDS (the CD4 count was 3 only) and the chest signs is due to Pneumocystis carinii pneumonia. To be honest, when the patient attended for her OGD, the diagnosis of AIDS had actually already been made. The gastric lesion had also been sampled and the pathologists reported: "non-specific specialised and non-specialised gastric tissue showing a variety of changes including oedema and haemorrhage with haemosiderin laden macrophages, with areas of solid spindle cells, vascular areas with small channels, and extravasated red blood cells". As you've guessed, the pathologists were clueless. This was because whoever took the original samples had not told them that the patient had AIDS (!) I took a second set of samples and this time told them about the HIV infection. Of course, this is all they needed and promptly did immunohistochemistry for "Kaposi's sarcoma-associated herpesvirus" (also known as; human gammaherpesvirus 8 or HHV-8 virus). Infection with this virus is thought to be lifelong, but a healthy immune system will keep the virus in check. In the immunosuppressed, the virus somehow get patients monocytes to express 'anti-programmed cell death protein 1' (PD-1) on their cell membranes, which inhibits apoptosis and cause 'immune escape' in several tumours. The checkpoint inhibitors nivolumab and pembrolizumab block PD-1 and have an antitumor effect. You'll recognise these two drugs because of the awful colitis they can cause. 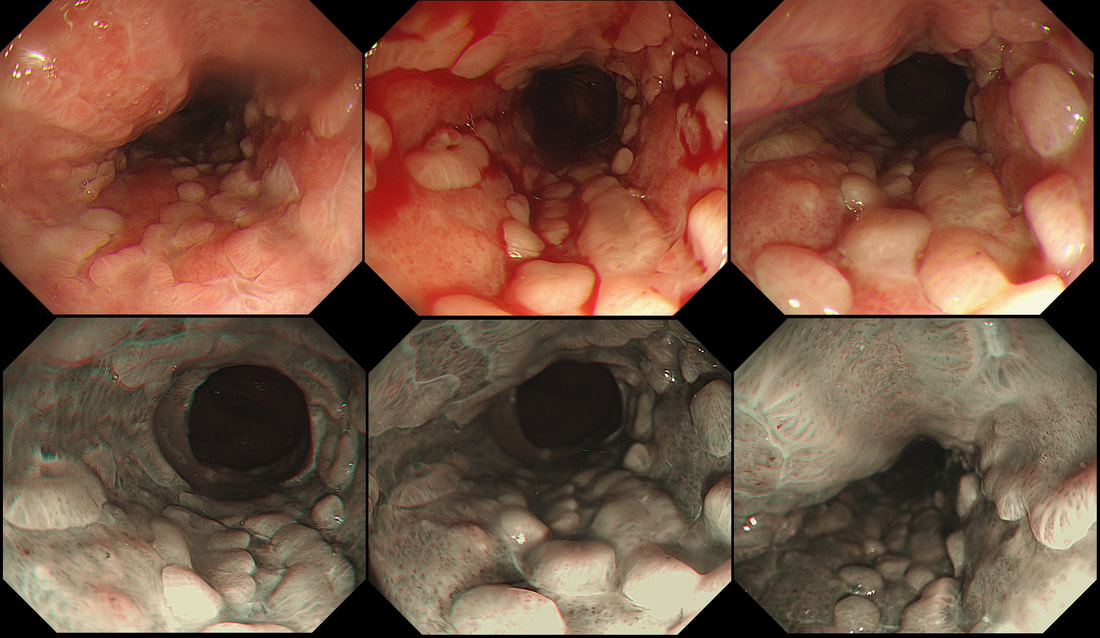 This is the oesophagus of a 45 yr old woman 3 weeks into induction chemotherapy for AML when she develops retrosternal pain and fever. Treatment with meropenem, ambisome, itraconazole, aciclovir and intravenous omeprazole is started with improvement of symptoms. This is the lower third of her oesophagus. WHAT IS THE MOST LIKELY DIAGNOSIS? a) reflux oesophagitis b) infective oesophagitis c) squamous cell carcinoma d) adenocarcinoma e) infiltration by myeloid cells explanation
An unusual appearance to the squamous portion of the oesophagus! Lower down, the appearances were unremarkable and healing reflux oesophagitis was therefore unlikely. Stains for fungi and immunohistochemistry for CMV were both negative. However, there were some multinucleated squamous cells and after a long search by our histopathologist, a couple of likely viral inclusions were found. This is a resolving herpetic oesophagitis ! Resolving because the patient had already been on aciclovir for a week when the endoscopy was done. Small miracle that our pathologists found traces of the original infection! This is a common issue with immunosuppressed patients. The haematologists are VERY quick to start a broad range of anti-microbial medication, covering fungi, viruses and bacterial pathogens. By the time the endoscopy is done, the original pathogen is usually suppressed to undetectable levels. This patient was brought down from the haematology ward with diarrhoea. The patient was immunosuppressed following a donor bone marrow transplant for myeloma. WHAT IS THE LIKELY DIAGNOSIS? a) Graft versus host disease b) An opportunistic infective colitis c) Checkpoint inhibitor colitis explanation
This is a case of acute Graft-versus-host disease (GVHD). Checkpoint inhibitor colitis gives a severe looking colitis whilst superficial ulceration is what should make you consider an opportunistic infective colitis. In the case of GVHD, there is usually very little to see. I knew that GVHD was due to T cells from the stem-cell donor which attack tissues in the recipient. However, I hadn't realised that it's the main cause of death after a stem cell transplant! This is bad news! The most common tissues affected by acute GVHD are the skin (widespread rash even appearing on the palms of the hands), liver (transaminitis) and the gastrointestinal tract. The horrendous secretory diarrhoea, classically developing in the weeks following a stem cell transplantation, is the most severe complication and linked with the 40% mortality rate of acute GVHD. There are a few take-home messages for endoscopists. ■ First, is that the mucosa may appear entirely normal but that samples nevertheless have to be taken as the diagnosis is clinical (of course) and histological (apoptosis of epithelial cells with loss of crypts). ■Secondly, endoscopic appearances are variable ranging from oedema (as in my video) to small intramucosal haemorrhages to erosions and ulceration. There is something called the 'Freiburg Classification' which basically orders this into a 4-level scale: 1 Normal mucosa 2 Patchy erythema 3 Aphthous ulcers and/or focal erosions 4 Confluent ulceration ■ Thirdly, 10 biopsies from the distal colon have the greatest chance of yielding the diagnosis. I take 3-4 biopsies from the rectum and sigmoid and if possible also the descending colon. ■ Fourth, because of the horrendous diarrhoea, there is no need to subject the poor patient to a phosphate enema before the flexible sigmoidoscopy. ■ Fifth, these patients often have low platelet counts and deranged clotting. Personally, I place an 11mm clip on each biopsy site to avoid the need for platelet transfusions and the need to correct the INR. However, this is a personal preference and for example the ASGE recommend bringing the platelet count up to above >50 × 109/L before biopsy (>20 for an endoscopy without biopsies). ■ Sixth, consider the possibility of superimposed infection, particularly if there is superficial ulceration as both CMV and HSV causes ulceration. Biopsies for viral cultures have to be placed in viral transport medium. Of course, the ward team should also have sent stool for viral PCR (adenovirus, astrovirus, rotavirus, noro-virus can all cause watery diarrhoea) as well as for bacterial pathogens such as C.diff and C. septicum as well as for parasites such as Giardia and Cryptosporidia Recently, I've had five referrals for GVHD. All patients were on high dose steroids (eg. 80mg of prednisolone) and in none of them did it seem to make any difference to their symptoms! All of the patients felt awful with abdominal pain, profuse diarrhoea and swollen limbs (from hypoalbuminaemia). Sadly, 2 out of 5 died within weeks of their flexible sigmoidoscopy. |