
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
This patient originally presented with a variceal bleed and was managed on ITU. Investigations confirmed alcoholic liver disease and the patient is entered onto a variceal ablation programme. At the first outpatient endoscopy, this is noted
WHAT IS THE LIKELY DIAGNOSIS?
explanation
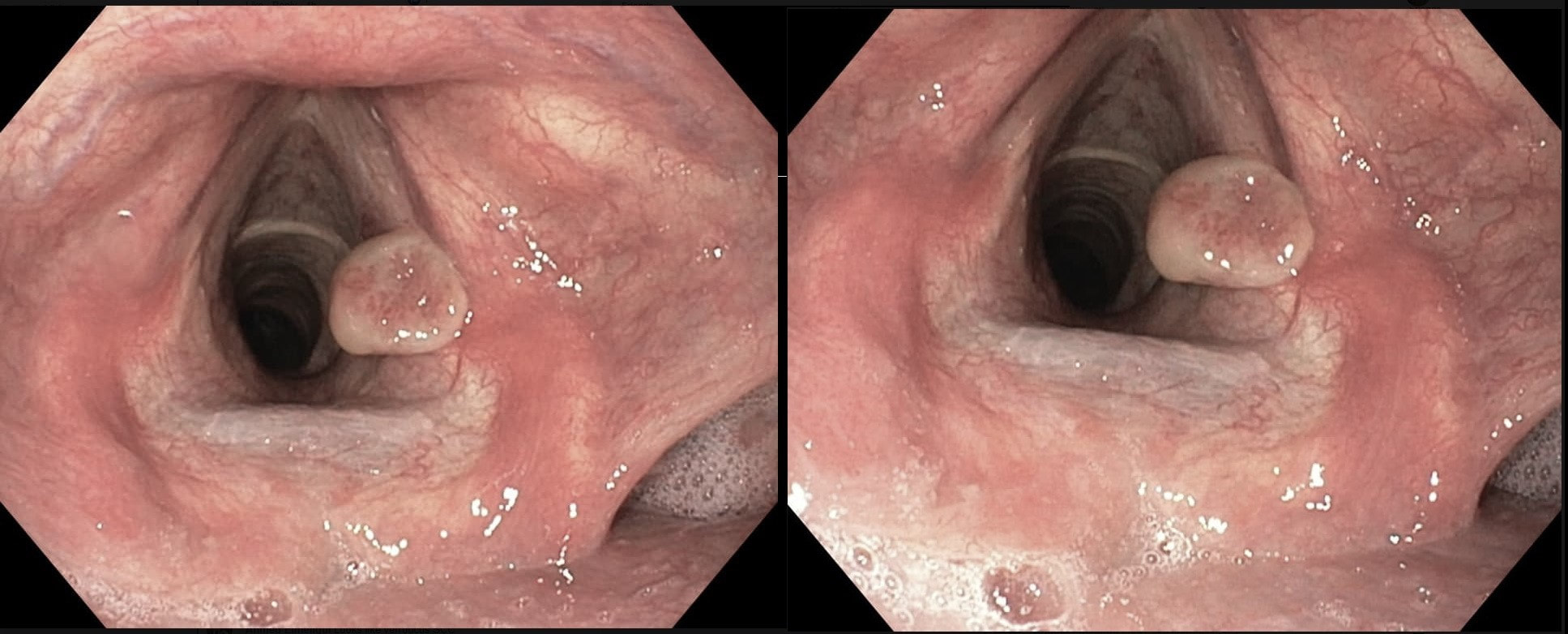
This is a vocal cord granuloma likely caused by irritation from the ET tube during the recent admission. Other causes include 'voice abuse', severe cough, vomiting, habitual throat cleaning, and the use of irritants such as tobacco and alcohol. Mucus cysts rarely develop on a vocal cord and look cystic rather than as granulomatous tissue as in this case.
Initially, management is supportive as these often shrink within 6-12 weeks. Surgery or laser ablation is reserved for large lesions but is a little fraught is these tend to recur unless to underlying cause is addressed. Singers should be advised to warm up the voice before singing (or speaking), resting the voice in anticipation of future speaking obligations and to avoid singing at times of an upper respiratory infection. This excellent photograph of a vocal cord granuloma was actually supplied by Dr Muslim Alkafaji who has been a member of Friends of Endoscopy since 2014 !!! This was an incidental finding in the pharynx WHAT IS THE DIAGNOSIS? explanation
This is a 'Pharyngeal retention cyst'. It was an incidental finding and the patient had no symptoms relating to this. These are the most common benign lesions in the pharynx, usually arising behind the epiglottis (the area is called the valleculae) or more to the side as here. The cysts are thought to result from dilatation of mucus glands secondary to retained secretions and chronic inflammation. They are usually incidental findings although larger cysts (>1 cm) may cause dysphagia, coughing or dysphonia. Complications include ulceration and secondary infections. This lesion was found in a 65 yr old man complaining of odynophagia. WHAT IS THE LIKELY DIAGNOSIS? explanation
There is a firm, disc-like indurated area on the right aryepiglottic fold. This turned out to be a T1 SCC which was ultimately treated by radiotherapy.
Of course, we should not ignore this area on intubation! Take a moment before irritating the larynx with the tip of your endoscope to look at the larynx! Is everything symmetrical? Your most common finding will probably be a yellow, submucosal 'retention cyst, thought to be the result of retained mucus within a dilated mucus gland. However, particularly in smokers, it's vital to include this part of the endoscopy in your examination. Sadly, no endoscopy reporting system accommodate for reporting findings in this area. This makes it particularly pertinent that you learn what the landmarks are called !!! See below for an update and don't get confused between left and right ☺ ! 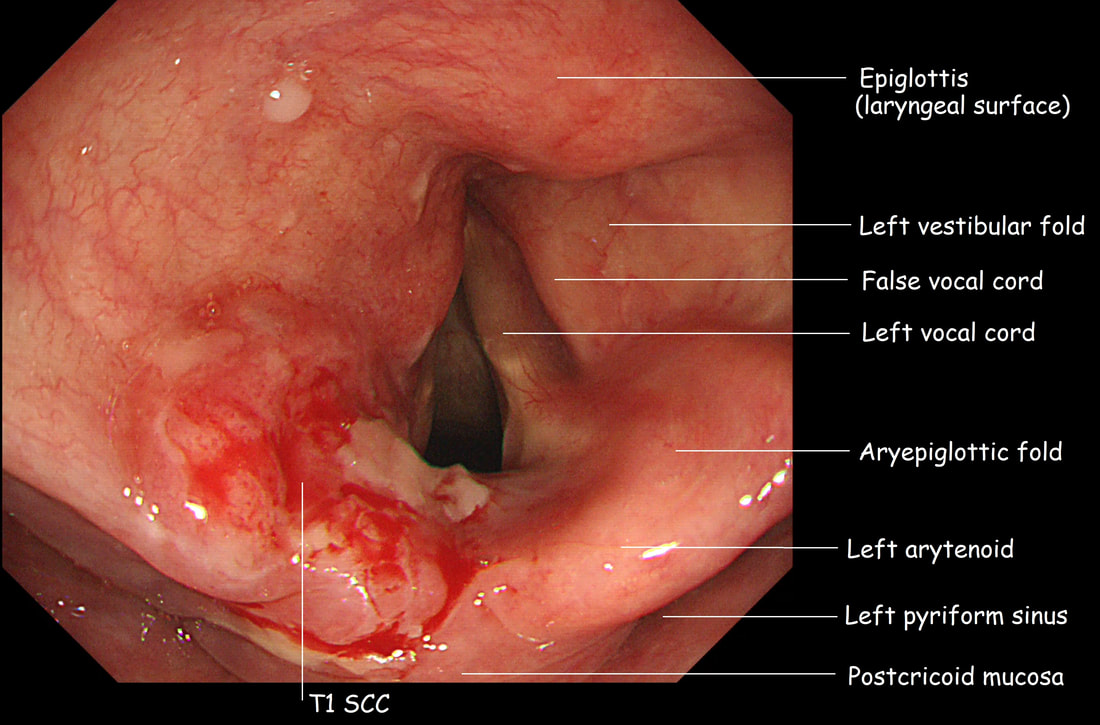
 A middle aged patient suddenly felt as he was choking and retched up this lesion to the horror of a nearby doctor. WHAT HAS THE PATIENT BROUGHT UP? Explanation
This beautiful, translucent polyp was sent for analysis and our pathologists rather drily reported: 'Nasal polyp'. With hindsight, I guess that any sort of fibrovascular polyp, dislodged from the oesophagus would have appeared more 'solid' than this semi-see-through polyp. However, you would have thought that the patient could have volunteered something like; " - I can breath better through my nose now", giving the hastily summoned doctor a clue ! |