
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
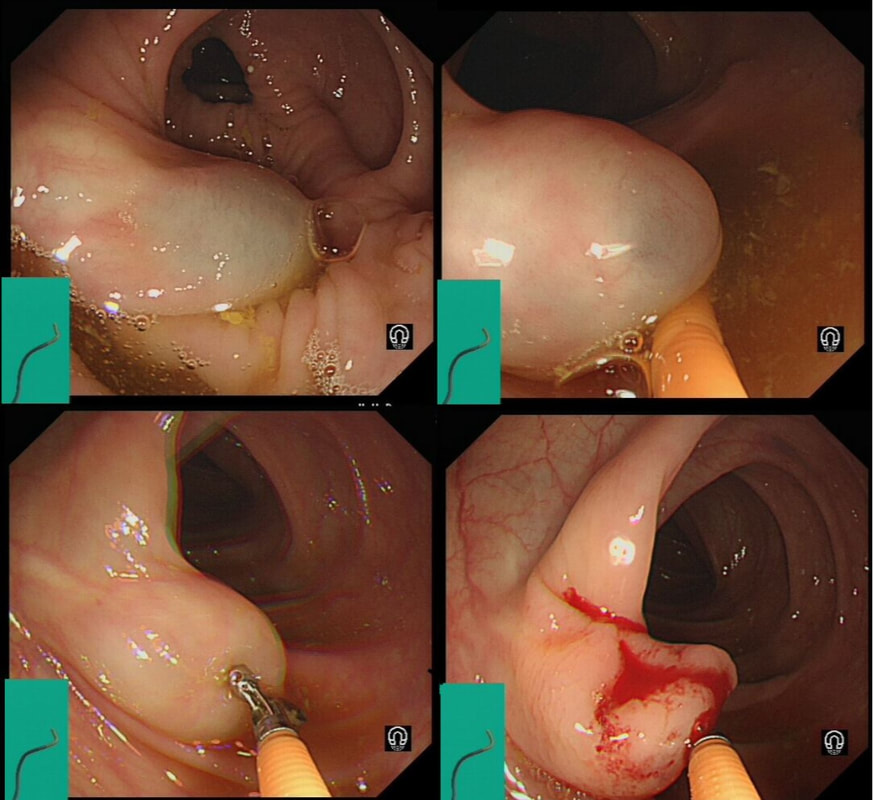
Just found another colonic lesion demonstrating the pillow sign.
WHAT IS THE DIAGNOSIS?
explanation
Just when I'd say that all lesions exhibiting the 'pillow sign', I realised that the exception are 'lymphangioectatic cysts' (lymphangiomas) !
These are thought to be developmental malformations which can be found anywhere in or on the body. Of course they are entirely harmless. In fact the only harm they cause is by being poked about! There has been a reported case of peri-colic abscess formation following biopsy [Krishna SG, Endoscopy. 2012;44(Suppl 2 UCTN):E104–5]. Therefore, either biopsy or a 'de-roofing EMR' should probably be avoided. The best way to confirm the diagnosis, if it's in doubt is by EUS. It will show several cystic spaces confined to the submucosa and without any nearby nodes. There have been reports of lesions presenting with abdominal pain, and when pedunculated endoscopic resection may be possible [Case Rep Gastroenterol. 2017 Jan-Apr; 11(1): 178–183]. Must admit that I remain a little sceptical. Each case would have to be assessed on its own merit I guess ! |