
|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
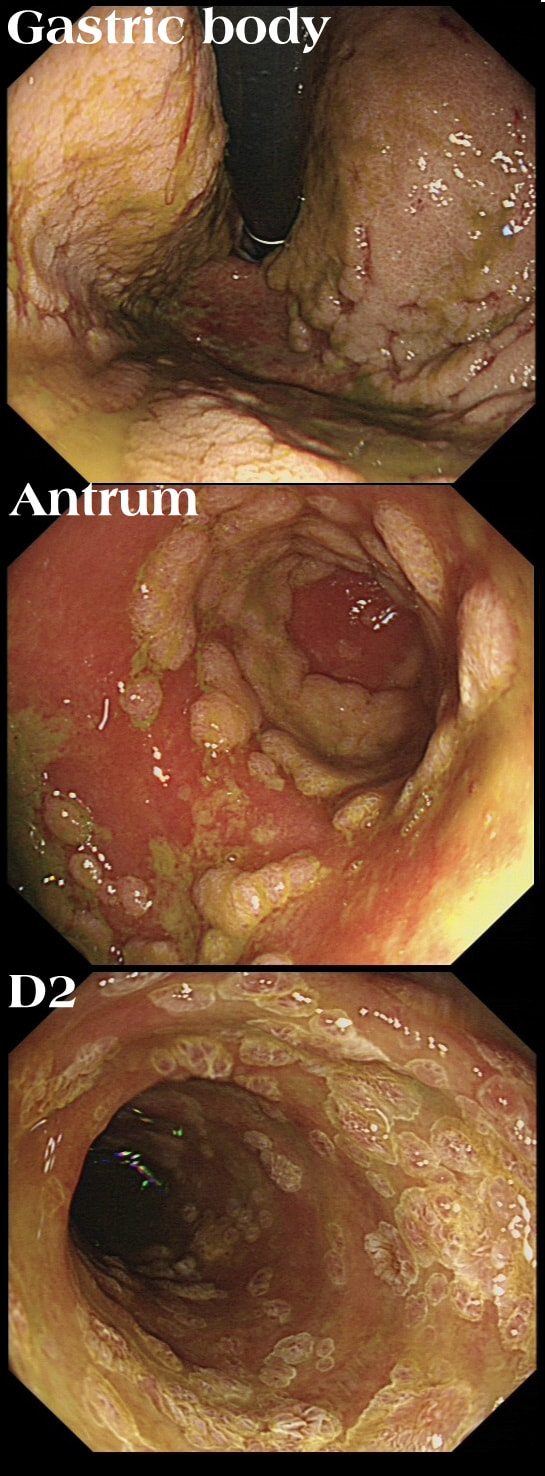
This patient has recently undergone a bone marrow transplant when she develops abdominal pain. PPI therapy has not improved her symptoms and she referred for a Gastroscopy
WHAT IS YOUR ENDOSCOPIC DIAGNOSIS?
explanation
Well this is a striking appearance! I'd never seen anything like it and tentatively suggested HSV gastritis on the histology request form. I didn't consider CMV because there was no mucosal ulceration.
Histology confirmed finding lots of oedematous CMV infected cells with granulation tissue and there was no need for immunostaining for cytomegalovirus proteins. This is a case of CMV gastritis! Actually, there were also some features suggestive of acute GVHD and I can therefore not be entirely sure that these 'plaque-like appearance on the mucosa isn't due to the combined effect of CMV+GVHD+PPI! It's not uncommon, one study, reported that approximately one-quarter of patients who were unresponsive to first-line acute GVHD treatment, actually had coinfection with CMV [Bone Marrow Transplant. 47, 694–699]. Of course, immunosuppressants is the trigger for CMV reactivation but CMV gastritis can occur in apparently immunocompetent patients, although a link with occult cancer has been suggested [Scand J Gastroenterol 2011;46:1228–35]. My guess of HSV was of course unlikely as HSV infects squamous mucosa or the colon (surprisingly), not the stomach. In the oesophagus you may see vesicles and/or small ulcers (left when the vesicles rupture). If I had seen this appearance in the colon I would have called this 'pseudomembranous colitis but of course C.diff doesn't affect the stomach. Can you get gastritis with checkpoint inhibitors? Yes, you can! It can cause a severe, haemorrhagic gastritis as outlined in this article [Case Rep Oncol 2018;11(2):549–556]. There is more information on CMV gastritis at this site. |