|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
|
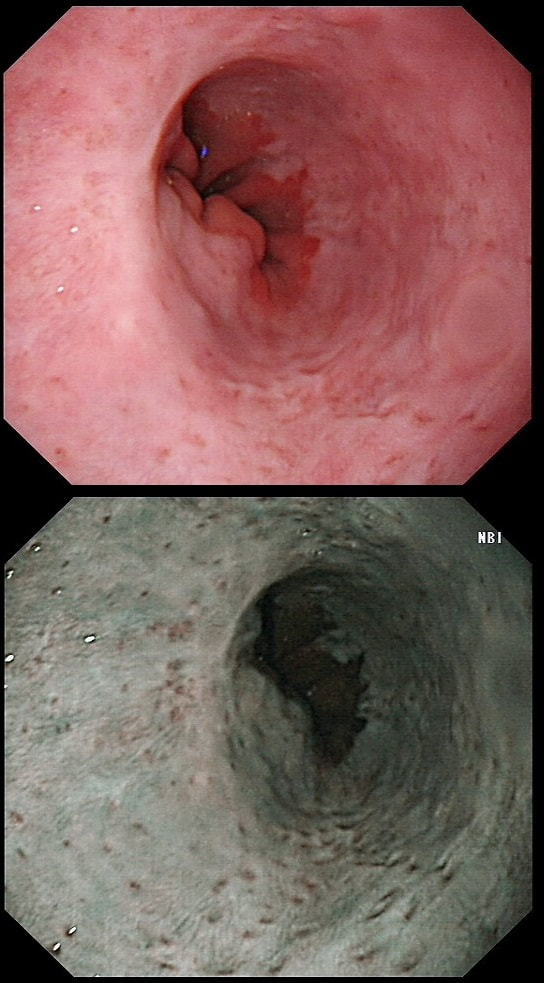
This is the GOJ of a 60 yr old woman with dyspepsia. WHAT IS YOUR DIAGNOSIS? Explanation
Actually, this patient was on a Barrett's surveillance programme. Five years earlier a small IMca had been removed following which annual surveillance had been reassuring. However, then this lesion was found and referred for removal.
Histological assessment of the resection fragment reported early invasion into the submucosa (which is 'allowed' provided that the depth of invasion is less than 500 microns (0.5mm). There was no LVI but unfortunately, there was poor differentiation. Of course, the 'worst' feature to find is probably LVI. Poor differentiation is worrying but less worrying than LVI. The reason for this is that 'poor differentiation' is a rather poorly defined entity. For example, how many crypts should be involved to call something 'poor differentiation' rather than 'focally poor differentiation'? Anyway, the patient was young and ultimately underwent an Ivor-Lewis which confirmed that the EMR had been curative with only some HGD remaining within the residual short stretch of Barrett's. We urgently need a prospective study following this type of Barrett's patient closely over time with regular EUS and CT to see if we can detect the small number of patients who subsequently turn out to have lymphnode involvement 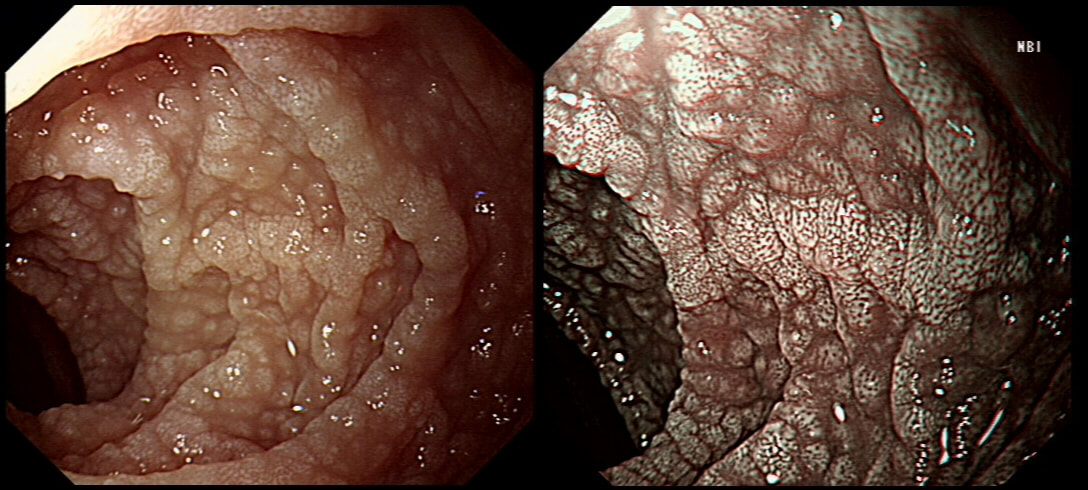
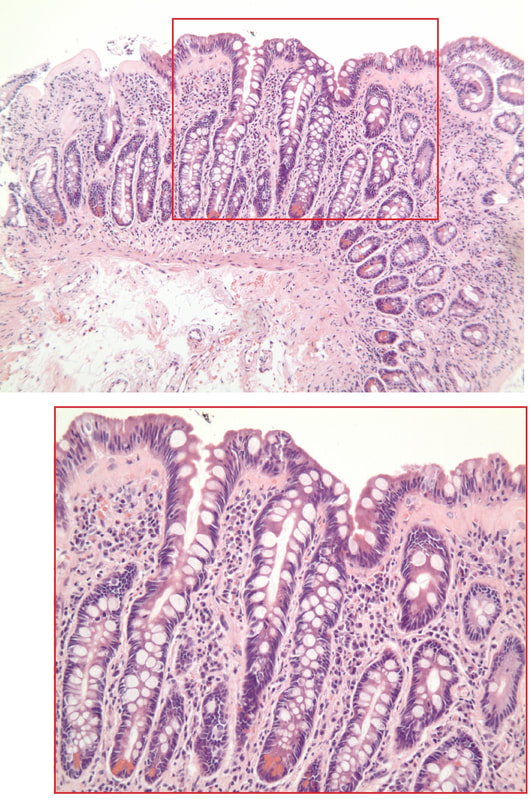
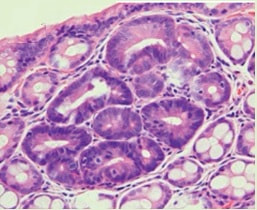
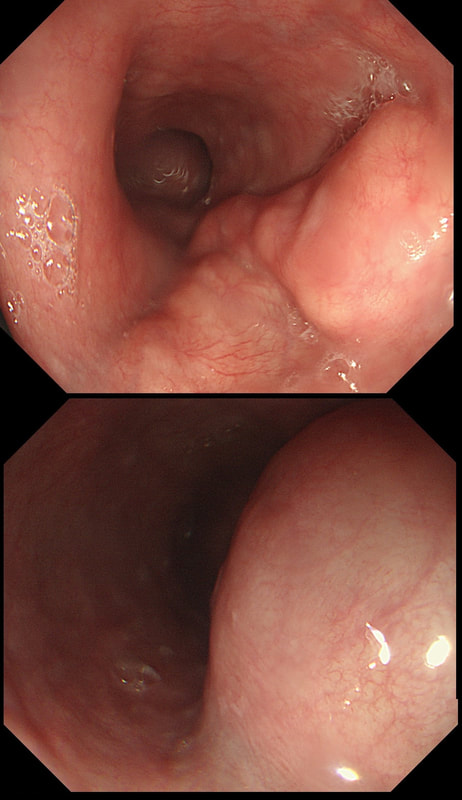
A middle-aged woman presented with loose stool and weight loss. Initially, she refused an endoscopy and a diagnosis of coeliac disease was based a high tissue transglutaminase (tTG) antibody titre. She was started on a gluten-free diet (GFD) but her symptoms remained despite adherence to the GFD. After several months she agrees to undergo an endoscopy. The images show the endoscopic view of the duodenal mucosa and the corresponding histology slide stained with haemotoxylin and eosin (H&E).
WHAT WOULD YOU DO NEXT?
explanation
Initially, the patient appeared to have classic coeliac disease, with diarrhoea and weight loss together with a positive serology. The endoscopy was crucial as the duodenal biopsies identified the presence of a thick band-like deposit of collagen just below the duodenal epithelium. On the basis of this finding, collagenous sprue was diagnosed.
Collagenous sprue was first described in 1947,1 but it was not until 1970 that Weinstein et al. introduced it as a diagnostic term to the medical nomenclature.2 Collagenous sprue is more frequent in females and in individuals who have other autoimmune diseases.3 It is now recognised that collagenous sprue shares similar clinical features with coeliac disease, such as chronic diarrhoea, anaemia and weight loss. In addition, the endoscopic and histological features of both diseases are similar, with an atrophic and scalloped duodenal mucosa. However, the histological hallmark of collagenous sprue is the presence of a thick subepithelial collagen band. Such collagen bands may also be found in collagenous gastritis and collagenous colitis.4 It has been proposed that collagenous sprue may be a heterogenous condition of collagenous gastroenteritides, including conditions such as collagenous colitis and coeliac disease.5,6 Unlike coeliac disease, in collagenous sprue, the typical histological changes may also be found in the stomach and colon.7 Furthermore, greater numbers of IgG4 plasma cells have been reported in the duodenal mucosa of patients with collagenous sprue when compared with the numbers in patients with coeliac disease, duodenitis or normal duodenal mucosa.8 As in our case, patients with collagenous colitis usually also have positive coeliac serology. For this reason, some believe that the collagen band is simply a marker of particularly severe coeliac disease, which may also be associated with ulceration, perforation and T-cell or B-cell lymphoma.9 An interesting report of paraneoplastic collagenous colitis was reported by Freeman et.al.10 In this case a patient with collagen deposits in both the small and large intestine was also found to have a coincidental colon cancer. After surgery, both the malabsorption and the histopathological changes completely resolved! For this reason, a search for underlying malignant disease should be considered. The response to a GFD is usually disappointing and for this reason, the outlook used to be grave for patients with collagenous sprue. However, remission of the condition has been reported with courses of corticosteroids11 or immunosuppressive agents such as infliximab.12 References
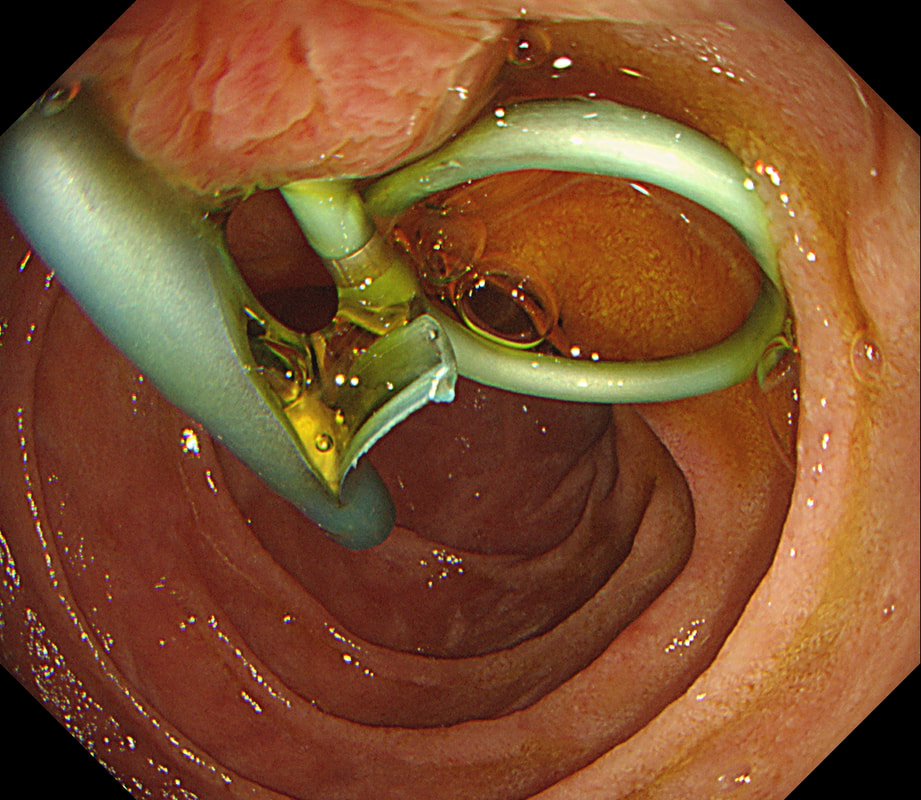
Patient has turned up to have his 'green' PD stent removed but I'm astounded to find two stents poking out of the papilla and they are both green !?
WHAT SHOULD I DO?
explanation
After scrutinising the X-rays, I concluded that the Pancreatic Duct stent was the 'single pig-tailed' stent (the one with the twist). Furthermore, the other one was draining bile. Obviously, the reason for the pig-tail is to stop the stent from migrating up the duct. PD stents are more likely to migrate than CBD stents and therefore the pig-tailed stent was more likely to be the PD stent even before I confirmed this on the images taken at the time of ERCP.
Well, this is one of the reasons why I don't like having stent removals on my list. Shouldn't it be the job of the person who placed to stent to also remove them?! This subcentimetere polyp was discovered in the rectum of a 60 year old woman undergoing a bowel cancer screening colonoscopy following a positive FIT. Considering the endoscopic appearance and the degree of lifting, WHAT WOULD YOU DO? explanation
That vein looks intimidating but don't be intimidated! It's not a 'show stopper'. it will move out of the way. However, that polyp does look nasty as there is no definite crypt pattern in the centre, just a swirly surface. However, the lifting is good, suggestive that we stand a good chance of clearing the lesion endoscopically ...
And at this point you can either go ahead and remove the likely early cancer. The advantage is that you get the correct diagnosis whilst biopsies are often inconclusive. The reason why surface biopsies are often unable to confirm invasive cancer is because your pathologists rely on seeing invasion of malignant tissue below the muscular mucosa. The underlying muscularis mucosa is usually NOT included in surface biopsies. However, this is a good example of the potential disadvantages of going ahead to resect the lesion. As you'll see in the video below, I removed it. Histology reported that the lesion was indeed an early rectal carcinoma, 6mm in diameter and with clear margins. However, the deep margin was 'only' clear by 200 microns which of course our pathologists would call a 'positive deep margin'. A 1mm (that is 1000 micron) is the 'accepted' definition of a 'clear surgical margin'. Secondly, there was of course a small focus of LVI. There is usually something to keep you awake at night after removing an early cancer. The disadvantage is obviously that you don't know what to tell the patient!!! - Is my cancer gone or not? - I'm sorry but I'm not sure! - Couldn't you keep a close eye on me with regular colonoscopies and CT's? Well, we could but there is absolutely no evidence that this will save your life IF you still have cancer cells inside of you... Fortunately, there is a study under way in the Netherlands to answer this very question! At the moment, we know that LVI is 'bad' and that the normal next step would be to offer the patient surgery. This is the sigmoid colon and rectum of a young patient who have just undergone bone marrow transplantation. WHAT IS THE LIKELY DIAGNOSIS? explanation
In GVHD there are minimal mucosal changes whilst there is extensive ulceration in this case. You do get nasty mucosal ulceration with checkpoint inhibitors but these drugs would not be used in transplantation. C.diff doesnt' cause mucosal ulceration and the herpes virus does not infect columnar mucosa. This leaves CMV ! Cytomegalovirus is a herpes virus that infects the majority of humans. Primary infection in individuals with normal immune function is usually asymptomatic or result in mononucleosis-like syndrome (fever, lymphadenopathy, and atypical lymphocytosis on a blood film). After primary infection, CMV becomes latent in various host cells but are controlled by a functioning immune system. When re-activation occurs in patients with severely compromised immune function (transplant patients or patients with AIDS and CD4 count <50 cells/microlitre), uncontrolled CMV replication can ensue leading to fever, bone marrow suppression, and tissue-invasive disease, depending on where the reactivated cells are residing. Investigations includes serology, pp65 antigenaemia test, histopatholical analysis of any tissue obtained, and PCR based detection. Treatment of choice is oral valganciclovir or intravenous ganciclovir whilst IV foscarnet and cidofovir are second line agents. 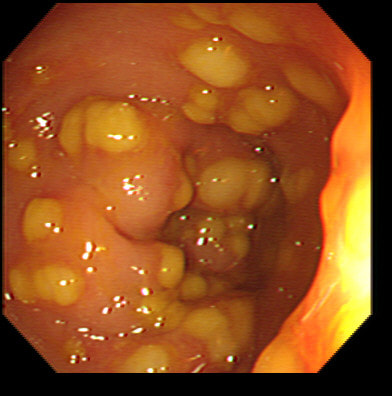
This is the sigmoid mucosa of an elderly inpatient who has developed diarrhoea.
WHAT SINGLE TEST WOULD YOU RECOMMEND NEXT?
explanation
Of course this is a case of Clostridium difficule associated colitis (pseudomembranous colitis). Patients usually present with diarrhoea, abdominal pain, and leukocytosis, and a history of recent antibiotic use. Other common symptoms include fever, abdominal tenderness, and distension.
In a symptomatic patient with typical colonic pseudomembranes such as in this case, arguably it would be sensible to recommend that treatment is immediately started. Stool testing should be considered in any patient with unexplained, new-onset diarrhoea (defined as 3 or more unformed stools in 24 hours in a patient not taking laxatives). Your local institution will probably have protocols for how patients should be investigated and all of the above test may well be part of the algorithm. When I was on the wards, toxin tests were favored over culture for diagnosis of C.diff because it was the toxins which mediate disease. detection of toxins was faster and correlated better with symptoms. However, there was a move towards 'molecular tests' (PCR for the bacterium) from 2009 because of concern that patients with C.diff could be missed by toxin tests. Of course, this raised the question; do toxin-negative patients with a positive C difficile PCR test result require treatment? Several studies have now indicated that about half of the patients with positive PCR test for C. diff do not experience adverse events without treatment and do not need treatment. For this reason, PCR testing for C.diff should not be used as the stand-alone diagnostic test. Instead it's patients with clinical disease (diarrhoea) AND a positive toxin assay who should be treated! There are lots of references for this statement and here is an open access article in JAMA: Treatment is to discontinue the responsible antibiotic and start therapy with oral vancomycin or fidaxomicin. Up to 50% of patients have a relapse after discontinuation of antibiotics, but most respond to a second course of therapy. In those who relapse again, faecal microbiota transplantation is very effective. This patient presented with an emergency GI bleed. WHAT IS THE DIAGNOSIS? explanation
There are actually several odd lesions in the stomach. Apart from the 'multi-focality', the lesions look a little like craters on the moon. Of course, this is what metastatic disease looks like. The dark colour clinches the diagnosis of melanomatous deposits. Here is a link to Sanjeev's and Ashok's case published in Digestive and Liver Disease [2020;52(12):1512] which is an even better demonstration of that dark pigmentation. Malignant melanoma has a peculiar predilection for the gastrointestinal tract. Melanoma can spread anywhere and is the most common metastatic tumor of the GI tract. More often the haematogenous spread is to the small bowel or colorectum. Gastric metastases are uncommon. It’s one of the more common findings in the small bowel of younger patients with anaemia. In an old post mortem series, the prevalence of GI metastasis in patients with melanoma was only 0.9% in 1000 melanoma patients (Arch Surg 1964:88:969-973). However, when you look at cases with advanced disease, up to 50% will have GI metastases (Cancer 1964;17:1323-39). As one may expect, the most common presentation is with anaemia or obstructive symptoms. Interestingly, surgical resection has been linked with a longer survival! Of course, its important to distinguish between a primary GI mucosal melanoma and metastatic melanoma. The criteria for a diagnosis of primary intestinal melanoma include 1) no evidence of concurrent melanoma or atypical melanocytic lesion of the skin, 2) absence of extra-intestinal metastatic spread of melanoma, and 3) presence of intramucosal lesions in the overlying or adjacent intestinal epithelium In a small series, the 5 year survival was 38% (Arch Surg 1996;131 :975-980). Without surgical intervention, the prognosis used to be grim and Amer et al. (Gynecol Obstet 1979;149:687-92) reported a mean survival time of 9.7 months, whilst others have reported an even shorter median survival of 4.7 months. Nevertheless, it is perhaps likely that case selection is the reason for the apparent survival benefit of surgery. The new checkpoint inhibitors and other immunotherapies are revolutionising the treatment of advanced stage disease. 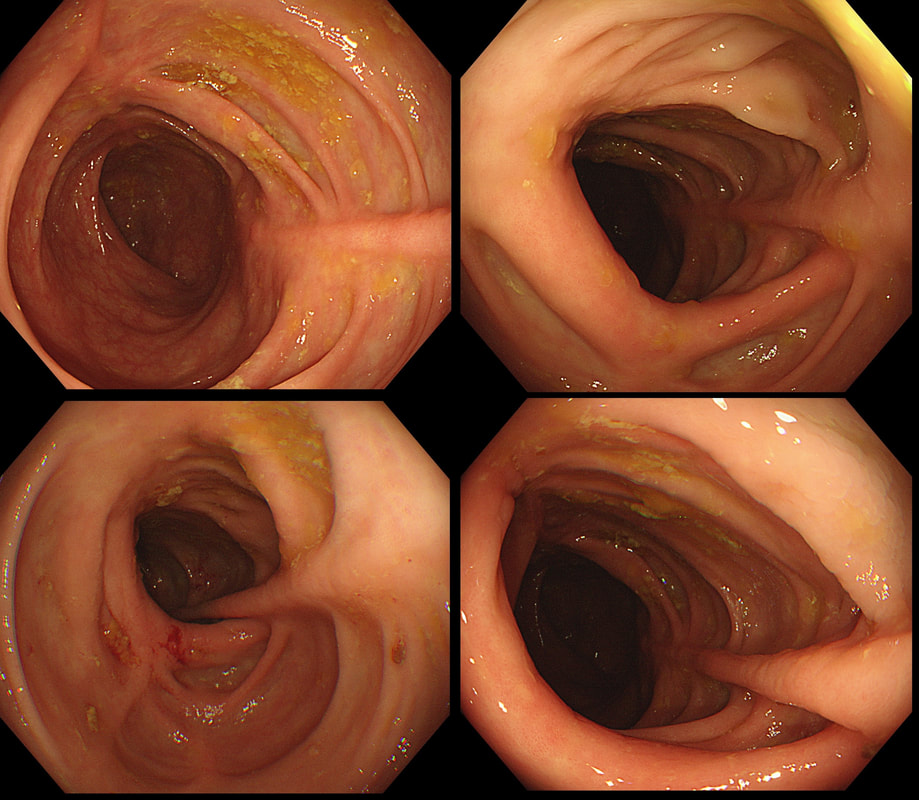
This is the colon of a 55 year old woman who has been treated for diarrhoea.
WHAT IS THE DIAGNOSIS?
explanation
Actually, this patient had collagenous colitis and after treated with budesonide, symptoms settled. A colonoscopy 3 months later showed these linear scars throughout the colon.
The first case of collagenous colitis was described in 1976 by Lindström and is characterised by chronic watery diarrhoea. Underlying hyperthyroidism, coeliac disease, bile salt diarrhoea and inflammatory bowel disease should be excluded. At colonoscopy, the mucosa is often unremarkable but there may also be mild, patchy erythema or linear cracks. Histology reveals thickening of the subepithelial collagen layer from the normal 3-6 μm to more than 10 μm as well as lymphocytic infiltration of the epithelium and the lamina propria (see image below). Rectal biopsies are not sufficient to make the diagnosis as normally the collagen layer is particularly thin here. Samples from the rectum and sigmoid confirms the diagnosis is more than 90% of cases. 9mg of Budesonide is effective but there is a high risk of relapse on stopping the drug [Bonderup OK. Gut 2003;52:248-51] and azathioprine is usually the second line agent. 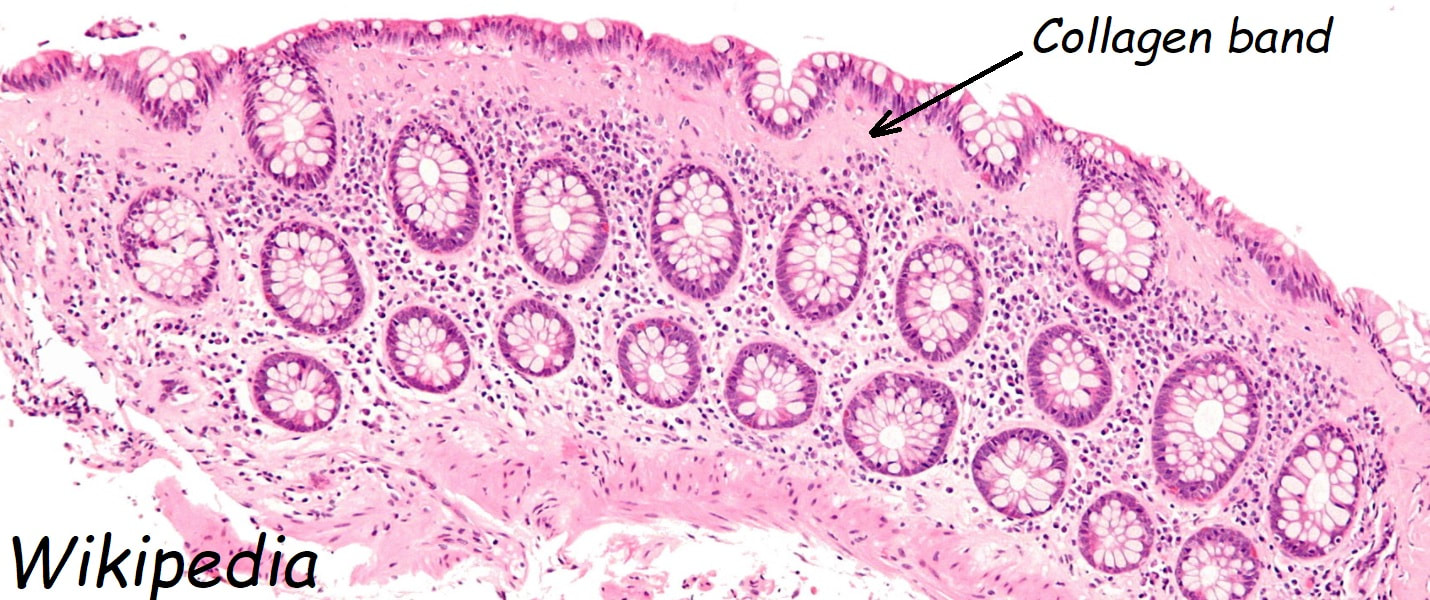
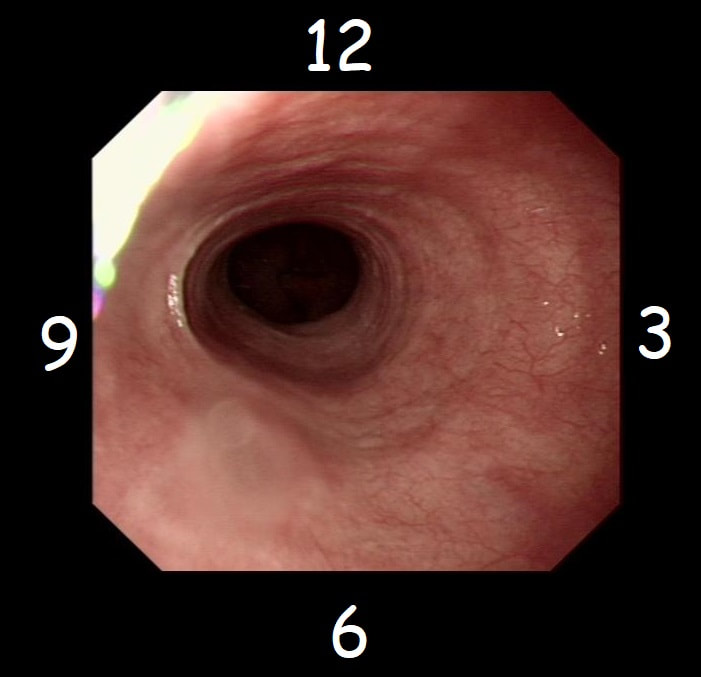
With POEM, knowing the landmarks outside of the oesophagus has become something which endoscopists are expected to be familiar with. Here is a quick self-test!
AT WHICH POSITION OF THE 'CLOCKFACE' DO YOU FIND THE:
explanation
Well the correct answers are:
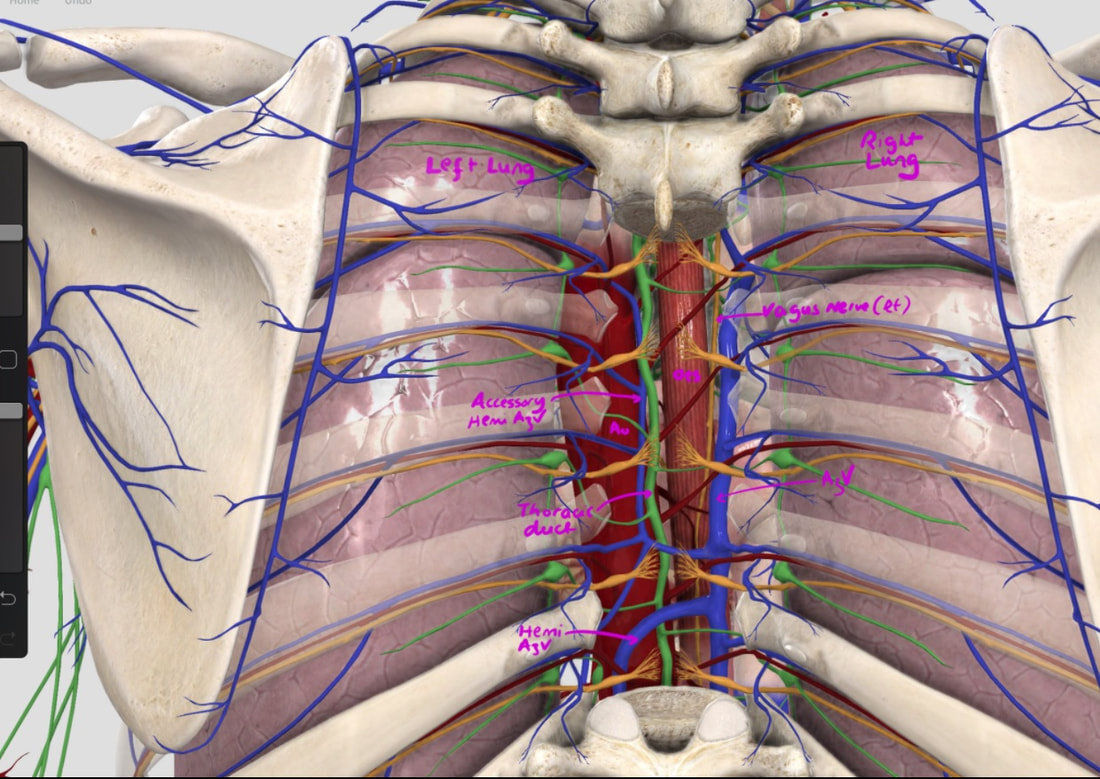
a) Spine - 6 o'clock b) Anterior vagal trunk - 12 o'clock c) Posterior vagal trunk - 6 o'clock d) Thoracic duct - 5 o'clock e) Left lung - 9 o'clock f) Aorta - 8 o'clock g) Azygous vein - 4 o'clock The images below tells the whole story! 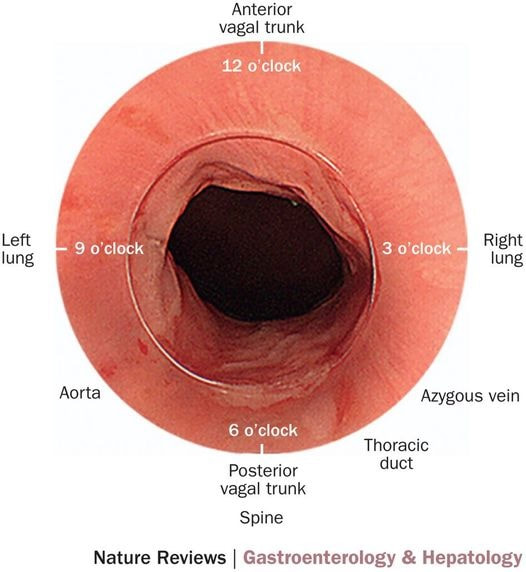
This lesion was found at the top end of the colon. WHAT WOULD YOU DO NEXT? explanation
This is a classical LST-G (laterally spreading tumour of the granular type). These lesions are always TVA's and almost always harbour LGD. Unfortunately, there are three problems which precluded an endoscopic resection; 1) there is a crazy alpha loop in the transverse colon which as usual proved impossible to remove, 2) the movement of the diaphragm continuously moves the lesion away and towards you and 3) the main part of the lesion is in the ascending colon but then extends across to the caecum where it almost kiss the appendix orifice. The moral of the story is to carefully consider BEFORE you start the resection. After you have started to attempt resecting a lesion such as this it becomes progressively more difficult to stop! It's like a gambler finding it increasingly difficult to walk away from the table as losses stack up. Because you have invested so much time and effort, it becomes difficult to stop and admit defeat! This was found in the sigmoid of a 35 year old lady presenting with abdominal pain and bleeding. She has been taking ibuprofen for her pain. WHAT IS THE MOST LIKELY DIAGNOSIS? explanation
The superficial, linear ulcers are typical of inflammatory bowel disease. Both ulcerative colitis and Crohn's disease can cause stricturing but of course Crohn's is more likely to. Those little nodules are post-inflammatory polyps, covered in normal crypts. In any case of colitis it's important to take a full set of samples, targeting not only areas which are visibly inflamed but also non-inflamed areas. Patchy inflammation is very suggestive of Crohn's disease but if you neglect to sample the non-inflamed areas, you will find that your pathologists will report a continuous colitis which would be more suggestive of ulcerative colitis. After all, they can only report on the samples given to them and may well not read your endoscopy report. 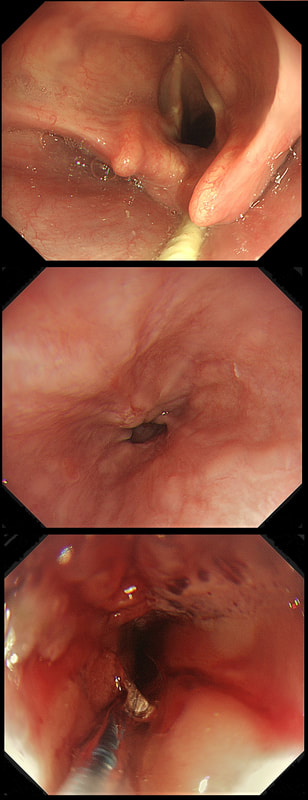
This 50 year old lady presents with dysphagia and a distal oesophageal stricture is confirmed. Intubation is a little tricky due to a pharyngeal pouch but we managed to intubate the oesophagus after the successful passage of a guidewire. After you have obtained a set of samples (last photo), the patient asks what will happen next.
WHAT IS YOUR REPLY?
explanation
The stricture doesn't look quite right does it? Somewhat 'nobbly' and without associated reflux oesophagitis. This stricture looks malignant ! There is one more concerning feature which you may have missed...
The vocal cord on the left-hand side is weaker than the right! On direct questioning, the patient confirmed that her voice had recently changed and become more hoarse! This patient had an advanced oesophageal cancer with metastases to the high lymphnodes on the left causing a recurrent laryngeal nerve paralysis! Out of the four options, organising a staging CT and referral to the UGI cancer MDT is the correct course of action! This 75 year old man underwent a CTC because of a change in bowel habit which has confirmed a large caecal polyp. The patient has been referred for a snare polypectomy. WHAT WOULD YOU DO NEXT? explanation
The location and the 'pillow sign' tells you that this lesion is a lipoma. We know from Shrisha Hebbar's Podcast that the ICV is a high risk location for any attempt at removing lipomas. He mentions a patient of his who presented with acute small bowel obstruction due to engorgement of an ICV lipoma after the placement of an Olympus ligation.
Furthermore, you wouldn't of course go ahead with an attempt at resecting a lipoma without due consideration of indications. How long has the patient had symptoms? Are they getting better? Are symptoms likely to arise because of this soft and floppy lesion. Probably unlikely and statistically speaking, this elderly patient is probably far more likely to have a change in bowel habit due to constipation. By the way, please take notice of the odd looking mucosal crypt pattern which is reminiscent of a TVA! This is the normal crypt pattern at the ICV at the transition to the villous surface in the terminal ileum! 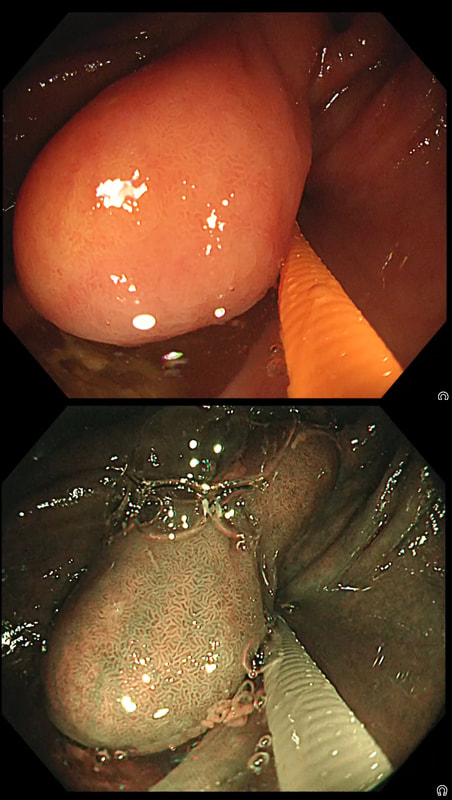
This patient has been referred for an oesophageal dilatation after biopsies have been reassuring WHAT WOULD YOU DO? explanation
Of course this stricture doesn't look right! There is a peculiar plaque-like area in the 10 O'clock position. The dilatation was cancelled and another set of samples were requested together with a CT. Samples indicated that this was a case of poorly differentiated intramucosal cancer and an EMR was organised. Have a look at the clip below. Clearly this lesion is firmly tethered to underlying structures and is beyond endoscopic cure. Some options may pop into your head such as injecting some fluid below the lesion or using the 'pull-within-the-snare' EMR technique. The problem is that these will not change the basic fact that endoscopically the lesion is beyond endoscopic cure! You run the risk of 'muddying the waters' with scrappy histology reporting 'intramucosal cancer at least' and with uncertain margins. Far better is to recognised the endoscopic irresectability of the lesion which provides a clear steer towards the 'next treatment level'. In this case the patient wasn't a surgical candidate and was offered chemo-radiotherapy (CRT).
The squamous portion of this oesophagus looks very unusual !
WHAT IS THE LIKELY REASON FOR THIS APPEARANCE?
explanation
This patient had undergone RFA, leaving the squamous mucosa looking a little odd. It's actually the openings of the 'oesophageal glands' which you can see. In my experience, there is no point in taking any samples as histology will be reported as normal. In most cases, Barrett's returns at the gastro-oesophageal junction. The return is slow and subtle and for this reason you should take samples from what appears to be the 'columnar side' of the squamo-columnar junction. As intestinal metaplasia (Goblet cells to you and me) are common at the cardia, the pathologists will not be able to tell you if the Barrett's is returning. However, they CAN tell you if the epithelium look dysplastic again!
In a minority of cases, perhaps 1:4 the recurrence happens below the squamous mucosa which can be very hard to see. Of course, the only way to deal with 'buried Barrett's', is to remove the patch by EMR! 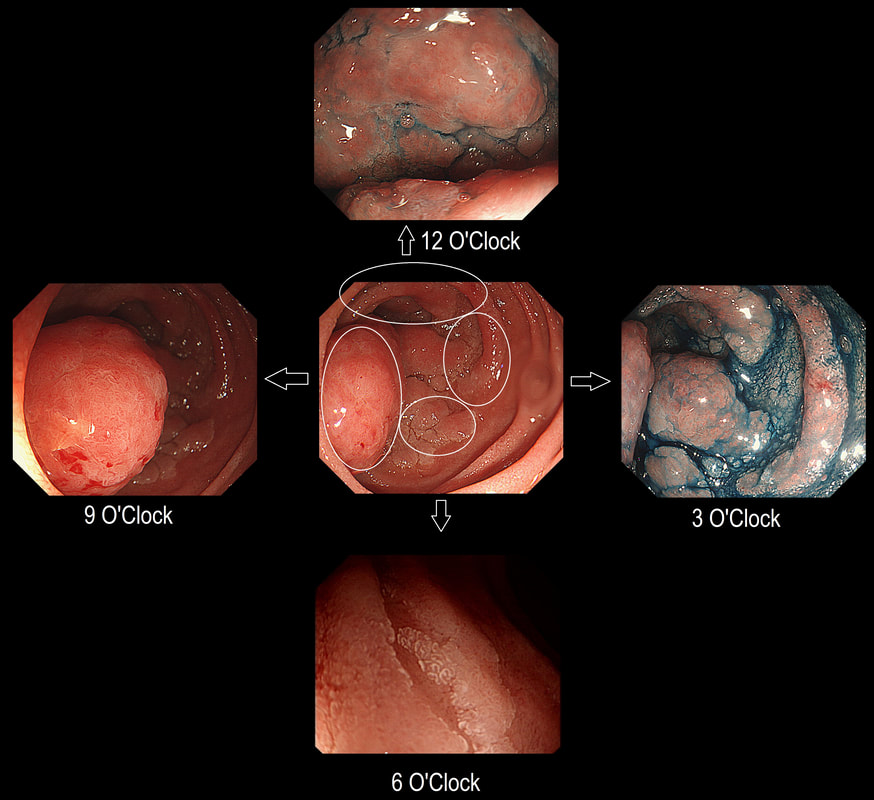
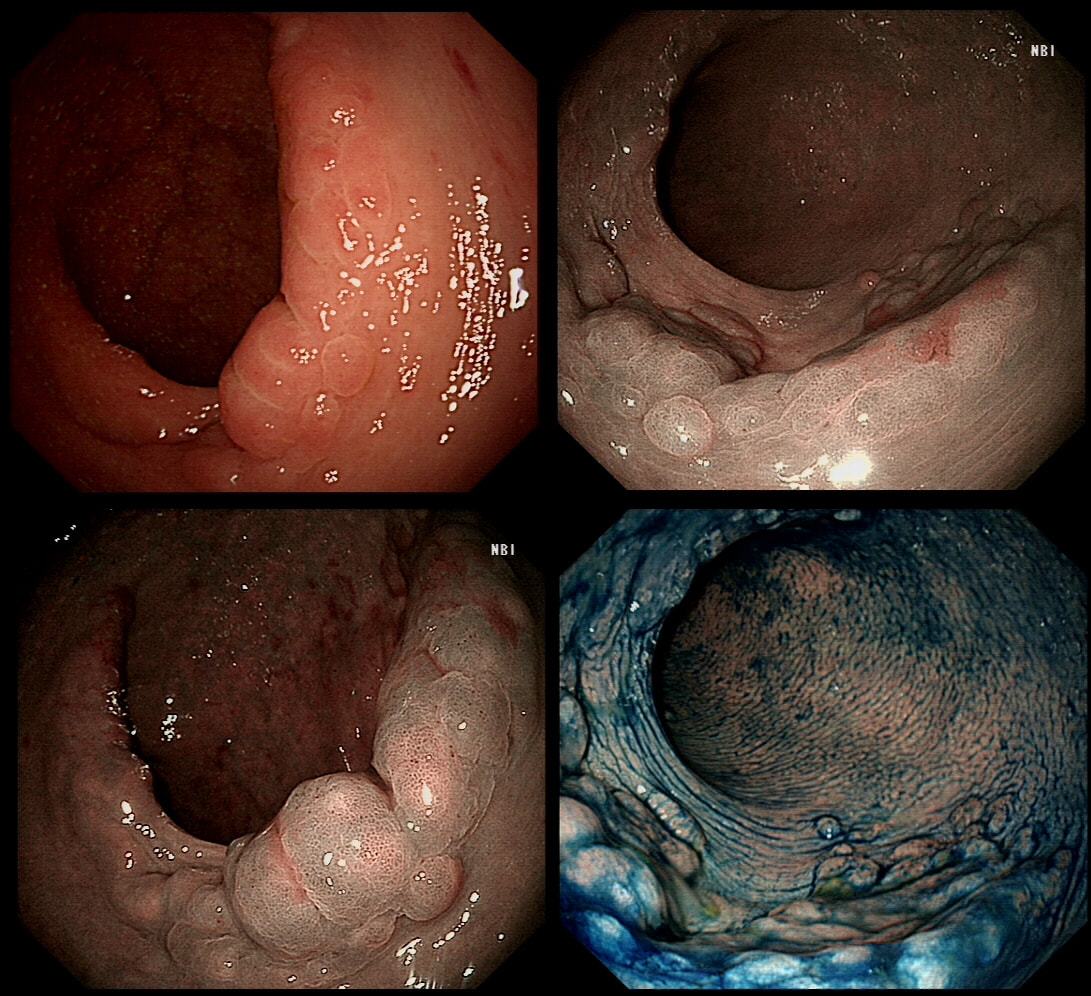
Here is a circumferential duodenal polyp situated in the second part of the duodenum. The patient is somewhat uncomfortable and your 'window of opportunity' is closing.
WHERE SHOULD YOU TARGET YOUR BIOPSY?
explanation
In general ampullary or peri-ampullary adenomas are far more likely to turn malignant than adenomas situated elsewhere in the duodenum. This is the first reason, why you should target your biopsy at 9 O'clock. There is a second reason and that is that the most 'chunky' polyp is at 9 O'clock. In my experience, the larger the 'polyp volume', the greater is the risk of malignant conversion.
So should we offer an ampullectomy? I would offer this to anyone with a life-expectancy of 10 years or more, I would consider (no promises) anyone with a life-expectancy of 5 years or more IF there is HGD on biopsies and there is no evidence of ductal obstruction (pt never had jaundice and there is no ductal dilatation or MRI or on EUS). Of course, an ampullectomy (probably better called a 'papillectomy') is dangerous but less dangerous than surgery. In Leeds we quote the following risks of a papillectomy: 1:10 risk of acute pancreatitis for up to a few months after the procedure, 1:10 risk of late bleeding for up to 2 weeks after the procedure, 1:50 risk of a perforation, a 1:10 risk of late papillary stenosis, 1:20 risk of acute cholangitis and a 1:200 risk of death Tiger country!!! 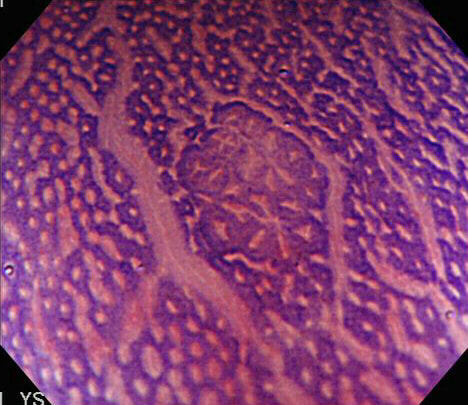
With a magnifying colonoscope and dye, another world is revealed.
WHAT IS SHOWN IN THIS PHOTOGRAPH?
EXPLANATION
The link between ACF and proximal adenomas, I see as evidence of a colonic “field effect” in which exposure to carcinogenic 'drivers' (dietary, lifestyle, disease and genetic) all work together to prime the colon for the development of cancer. It's for this reason, that endoscopically resecting DALM's (I arbitrarily define DALM's as flat polyps within the colitic field of a patient with >6 yrs of colitis), then telling patients that they now have nothing to worry about, is naïve ... 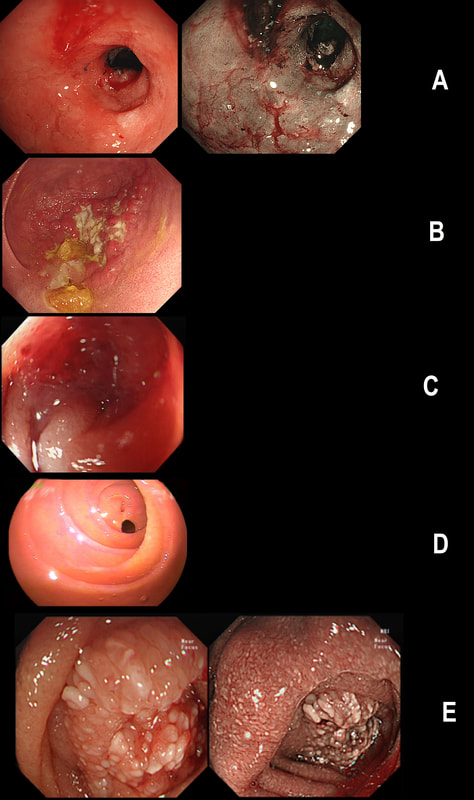
Just another piece of fun ☺! Here are 5 photographs of duodenal strictures, each of a different aetiology!
CAN YOU MATCH THE STRICTURE WITH THE PHOTO?
EXPLANATION
You'll know that NSAID induced strictures are classically 'membrane-like' as in Photograph D.
The 'Peptic stricture' is shown in photograph A. The healed duodenal ulcer had been at 9 O'clock in that stricture. Chronic pancreatitis causes external compression of D1 or D2 usually with swollen villi. Of course there are two photographs to choose between - Photo C or E. Lets leave that one and see if the Crohn's stricture is easier to find. Of course, photograph B shows ulceration and inflammation and must be the CD stricture. That leaves the malignant stricture which could be photograph C or E. It's usually relatively easy to squeeze past the external compression caused by a swelling in the head of the pancreas. In contrast, malignant duodenal strictures are usually impassable. Which one looks the tightest? Photo C or E? Well, C is the malignant stricture which I had to dilate up to 10mm before I could take samples a little deeper into the stricture to confirm the diagnosis. Photograph E was a case of severe pancreatitis which we scoped as he had dropped his Hb (never found out why or how). 

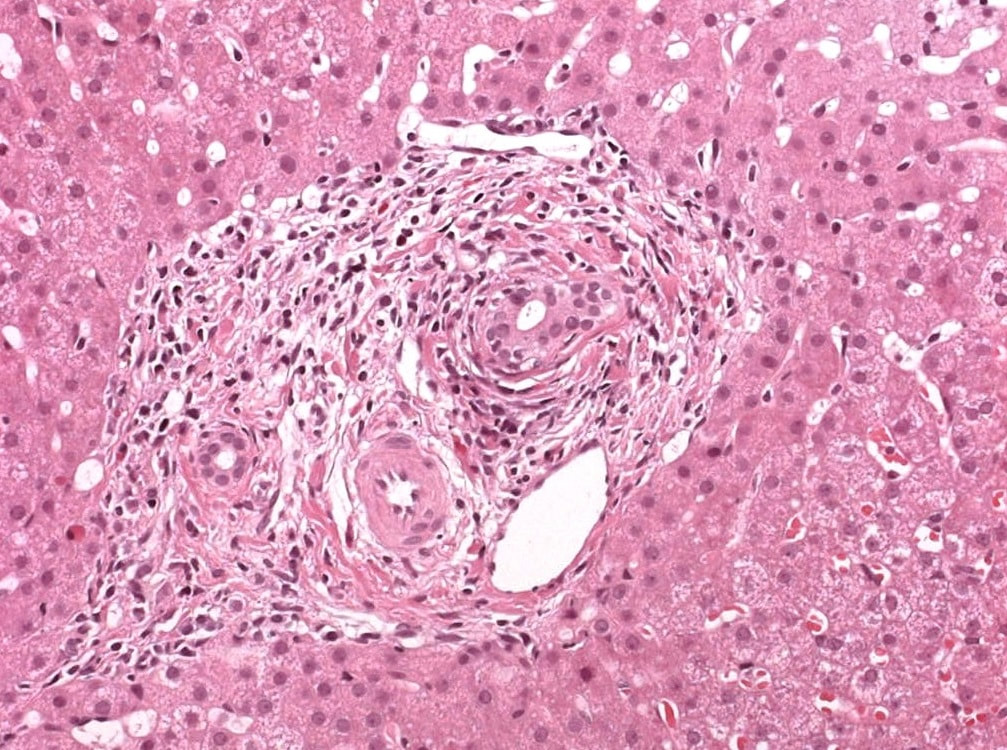
A full house of cholangiogram, cholangioscopy and histology of a 35 year old man with jaundice!
WHAT IS THE DIAGNOSIS?
explanation
This is of course something of a curveball. Why would a patient with any of these causes of jaundice undergo an ERCP? Surely a clinical assessment, blood tests and an MRI would be the investigation of choice? Without any risk of giving the patient cholangitis!? Actually, the three images (cholangiogram, cholangioscopy and histology) are from three historical cases ☺!
MRI has a sensitivity of about 85% and specificity of around 95% for PSC. In most cases of PSC (87%), both intra and extra-hepatic bile ducts are involved , intrahepatic ducts alone in 10-25% and very rarely only the extrahepatic ducts (2%). Cholangioscopy shows patches of inflammation on the wall of the CBD and the cholangiogram did suggest some 'pruning' of the intra-hepatic biliary tree. A subsequent liver biopsy (we really did go all out), shows the typical peri-portal 'onion skin' inflammatory changes in keeping with PSC (although histology can't usually completely rule out other causes of biliary obstruction). 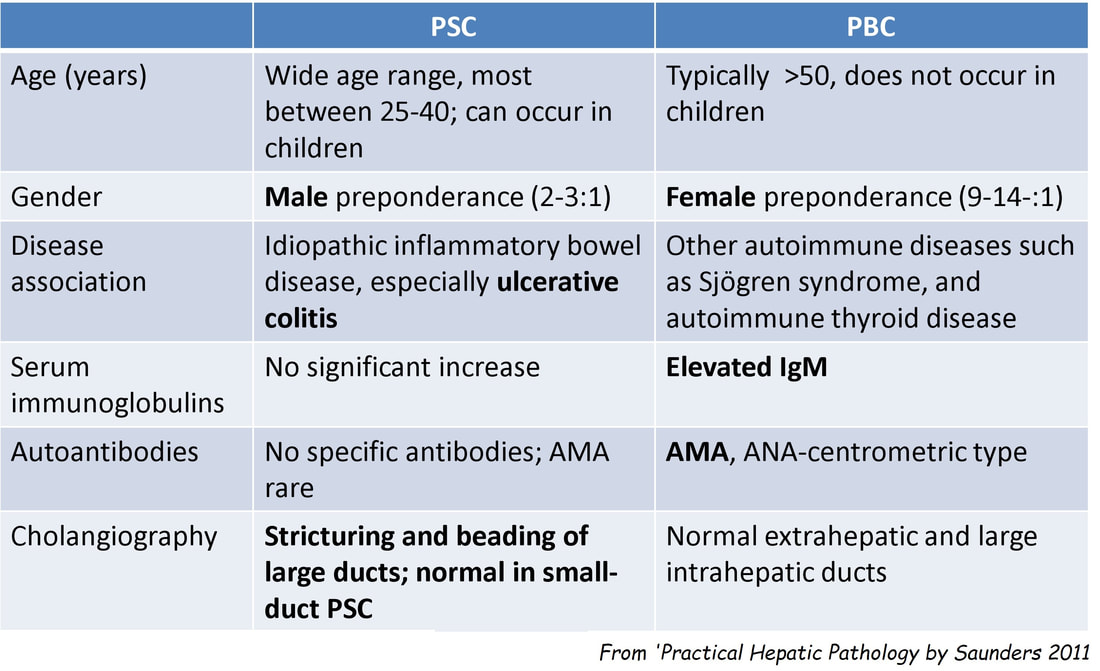
This video clip requires no introduction. No other abnormality was found. WHERE IS THE LIKELY SITE OF THE PROBLEM? explanation
Quoting the 'Sarin Classification' of gastric varices, this is a case of an 'isolated fundal varix' (IGV1). In this case the underlying cause was splenic vein thrombosis following an admission for acute on chronic pancreatitis. The precise distribution of the varices helps you to pinpoint the location of the thrombus. The infographic below from Song et.al is brilliant:
Briefly, 1) oesophageal varices with or without fundal varices points to portal vein thrombosis 2) fundal varices ALONE points to splenic vein thrombosis 3) antral and/or duodenal varices points to a thrombus in the gastro-epiploic vein Brilliant ! 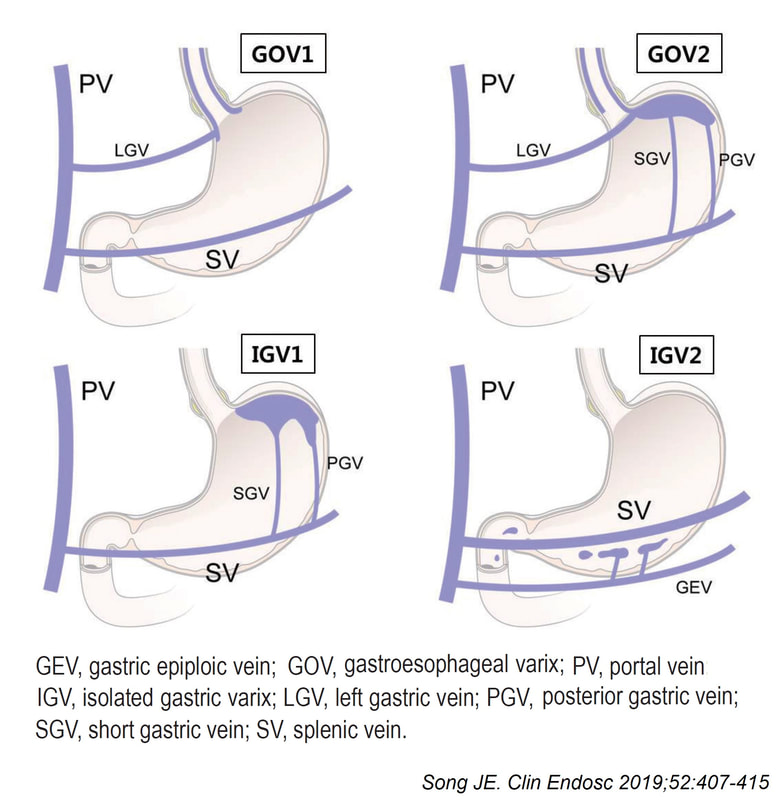
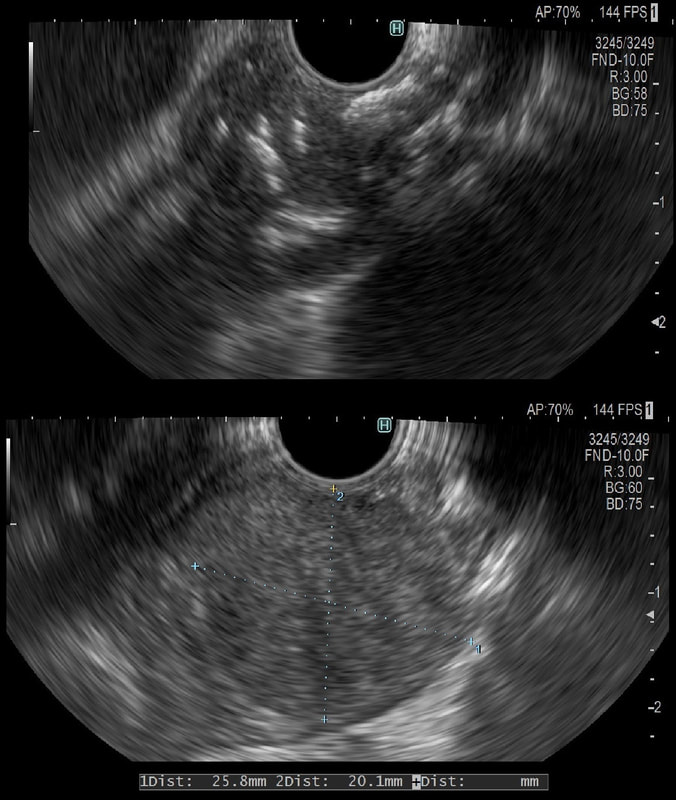
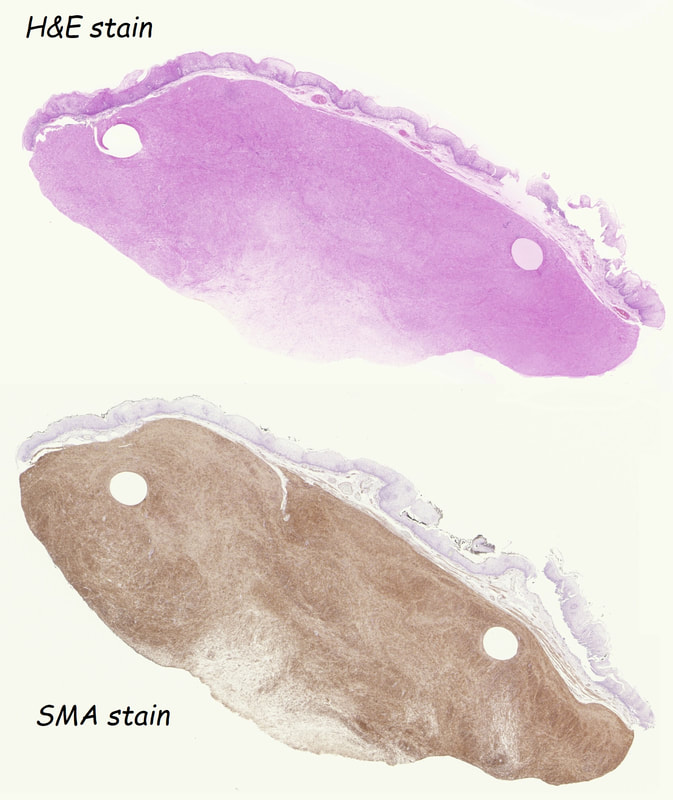
This was an incidental finding in the mid-oesophagus. Subsequently an EUS is organised and the lesion is ultimately removed (histology in the last image)
WHAT IS THE DIAGNOSIS?
explanation
Leiomyomas are the most common submucosal lesion found in the oesophagus. No idea why they are so rare in the stomach, where GIST's are the most common submucosal lesion. Correspondingly GIST's are very rare in the oesophagus.
These usually arise from the circular muscle propria layer. On CT they are often calcified and there are of course no nearby nodes to suggest malignant disease. Indeed, malignant transformation is extremely rare and for this reason many centres would ignore a small submucosal lesion such as this, when found in an elderly person. Larger (around 5cm usually) and symptomatic lesions (which are more likely to be leiomyosarcomas) are enucleated surgically. "- They shell out like peas" according to one of our UGI surgeons. However, our local surgeons are also careful to point out that resection usually result in some damage to the muscle propria layer, which require repair as otherwise a diverticulum may develop. With endoscopists spending more time in the 'third oesophageal space' (i.e. the submucosal space), doing ESD's and POEM, the suggestion that we should also remove leiomyomas endoscopically has arisen. May seem like a good idea but I would advocate caution for the simple reason that endoscopically, we are unable to repair the defect we cause in the muscle propria layer ... Oh, how about that 'SMA stain' used in the histology. This is 'Smooth Muscle Actin' stain which does exactly what it says on the tin ... 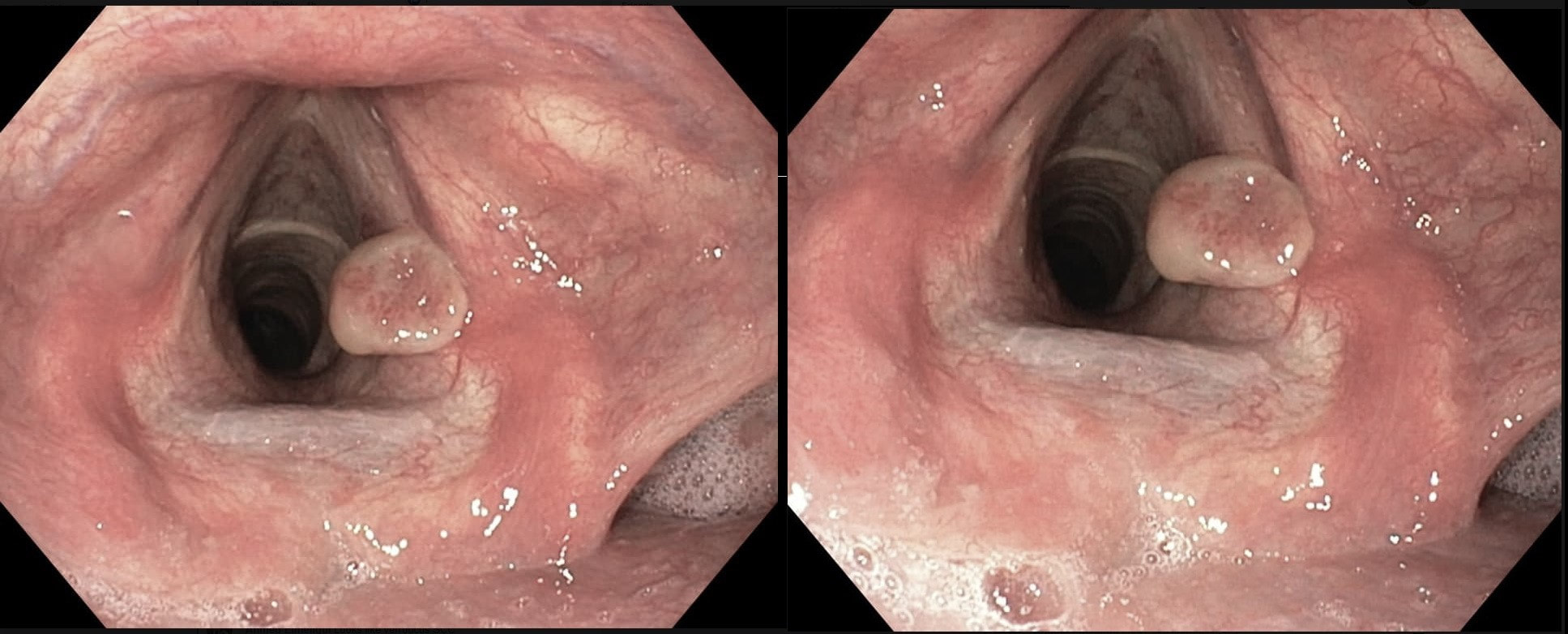
This patient originally presented with a variceal bleed and was managed on ITU. Investigations confirmed alcoholic liver disease and the patient is entered onto a variceal ablation programme. At the first outpatient endoscopy, this is noted
WHAT IS THE LIKELY DIAGNOSIS?
explanation
This is a vocal cord granuloma likely caused by irritation from the ET tube during the recent admission. Other causes include 'voice abuse', severe cough, vomiting, habitual throat cleaning, and the use of irritants such as tobacco and alcohol. Mucus cysts rarely develop on a vocal cord and look cystic rather than as granulomatous tissue as in this case.
Initially, management is supportive as these often shrink within 6-12 weeks. Surgery or laser ablation is reserved for large lesions but is a little fraught is these tend to recur unless to underlying cause is addressed. Singers should be advised to warm up the voice before singing (or speaking), resting the voice in anticipation of future speaking obligations and to avoid singing at times of an upper respiratory infection. This excellent photograph of a vocal cord granuloma was actually supplied by Dr Muslim Alkafaji who has been a member of Friends of Endoscopy since 2014 !!! 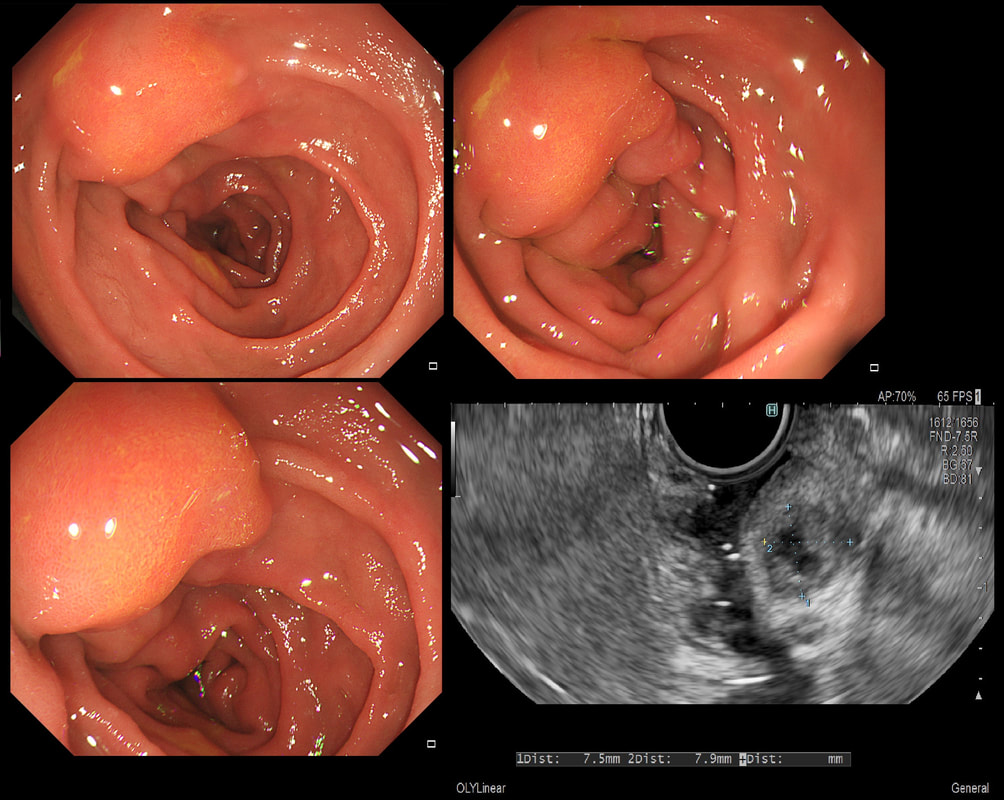
This 25 year old man presented with an attack of jaundice. Here are photographs of his duodenal ampulla and EUS
WHAT IS THE DIAGNOSIS?
explanation
That EUS does confirm a cystic dilatation of the distal part of the common bile duct. Of course, the patient has a 'choledochal cyst' ! These are congenital cystic dilatations of parts of the biliary tree. In this case, only the distal CBD was involved, making this a 'type III' choledochal cyst which is located at the ampulla (see figure below).
Most cases presents as jaundice or pain in infants. Chronic cholestasis may present later with biliary cirrhosis or cholangiocarcinoma. Fortunately, this case was discovered before cirrhosis and the patient was treated with surgery. 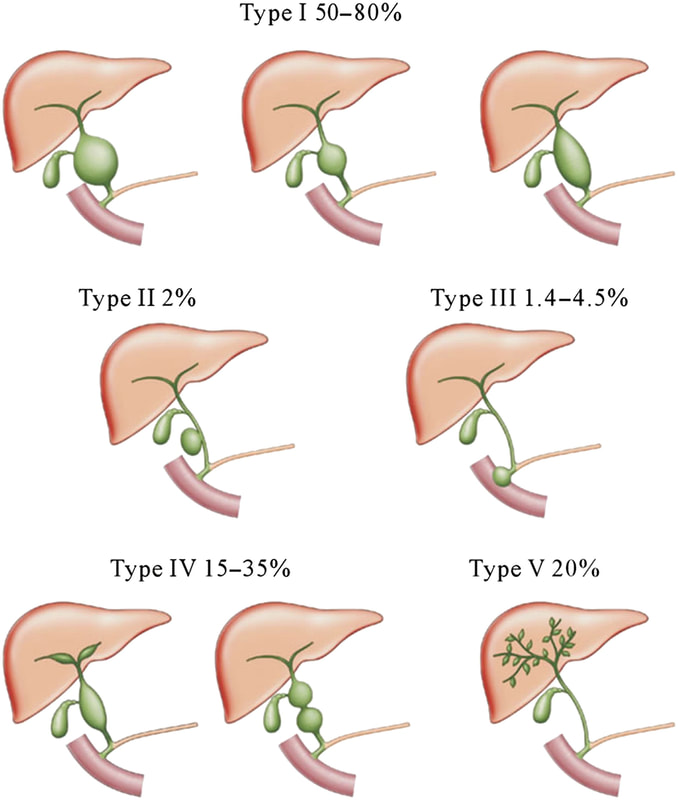
I found this in the low rectum of an elderly lady undergoing a flexible sigmoidoscopy because of rectal bleeding. A quick check with the patient confirmed my suspicions.
WHAT IS THE DIAGNOSIS?
explanation
On first glance this looks like a circumferential serrated polyp in the rectum. Of course, this would be somewhat odd and furthermore, unlikely that the patient would know anything about this.
Actually, on direct questioning she did know about her prolapse! Another common endoscopic finding is an erythematous and oedematous patch, close to the anal margin. 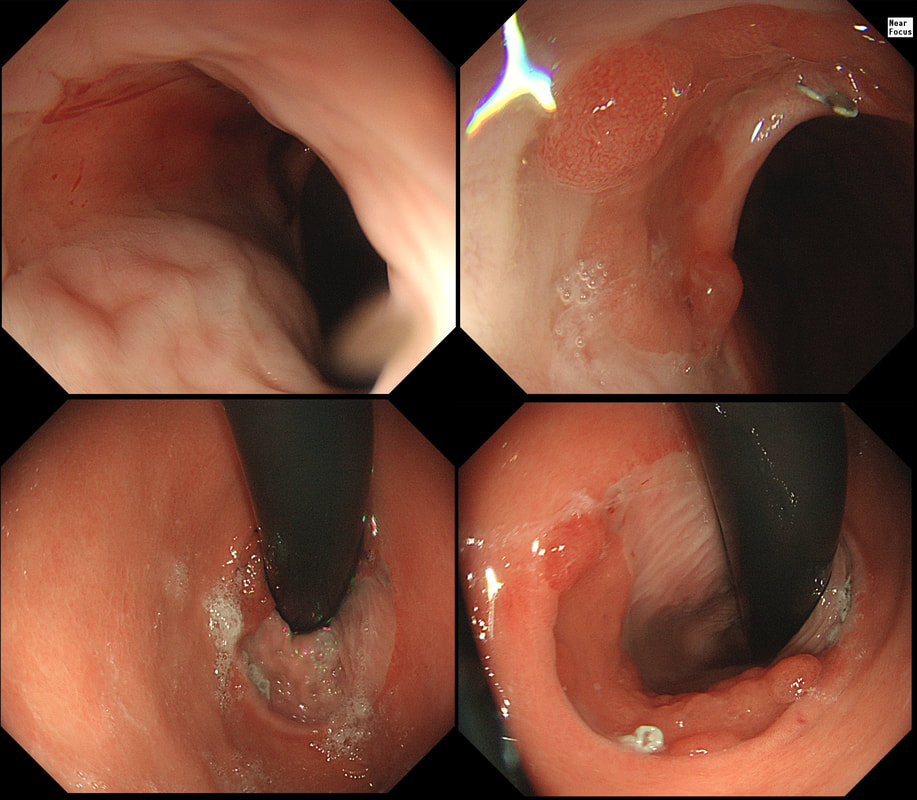
This is something of an enigmatic image of significant problem. It may not look like a problem ..
WHAT DOES IT SHOW?
explanation
The trick is to work out what's happened! Of course, this patient has undergone an 'Ivor-Lewis' oesophagectomy for oesophageal adenocarcinoma. Unfortunately, the surgical anastomosis between the mid-oesophagus and the 'gastric tube' wasn't quite high enough and the surgeon has left a small patch of Barrett's behind. Potentially a ticking time bomb !
Fortunately, it should be possible to remove this small patch of Barrett's by either an EMR or RFA. I think that the Barrett's is a little too nodular (histology reported LGD), and we therefore opted for an EMR rather than RFA. |