|
Friends of Endoscopy is all about pattern recognition. See it today and recognise it tomorrow! Learn from a New Case on most weekdays !!!
Become a Better Endoscopist ! |
|
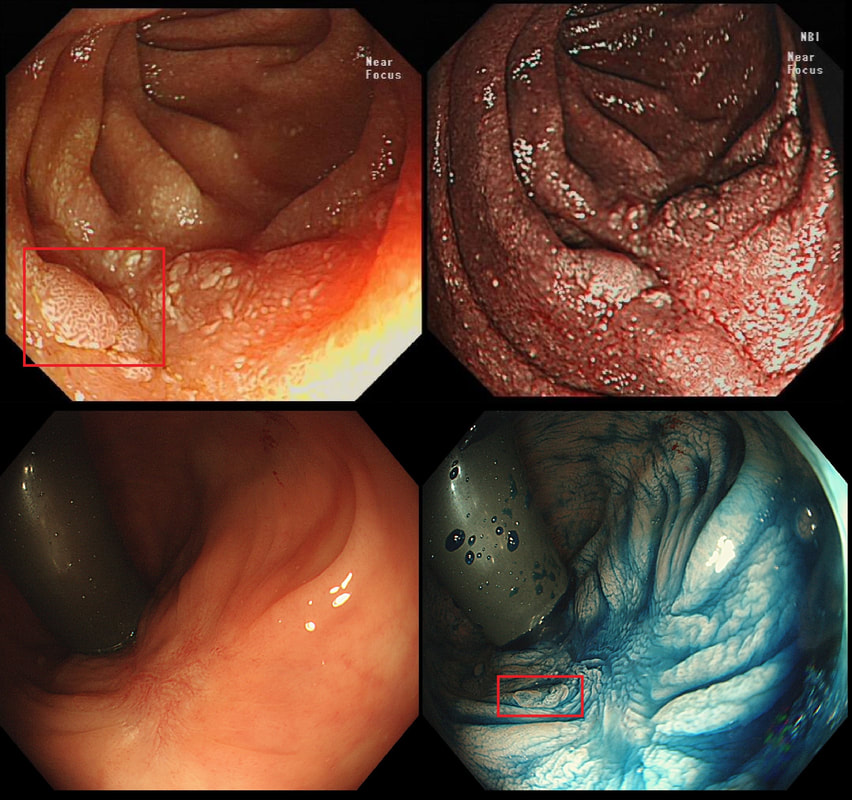
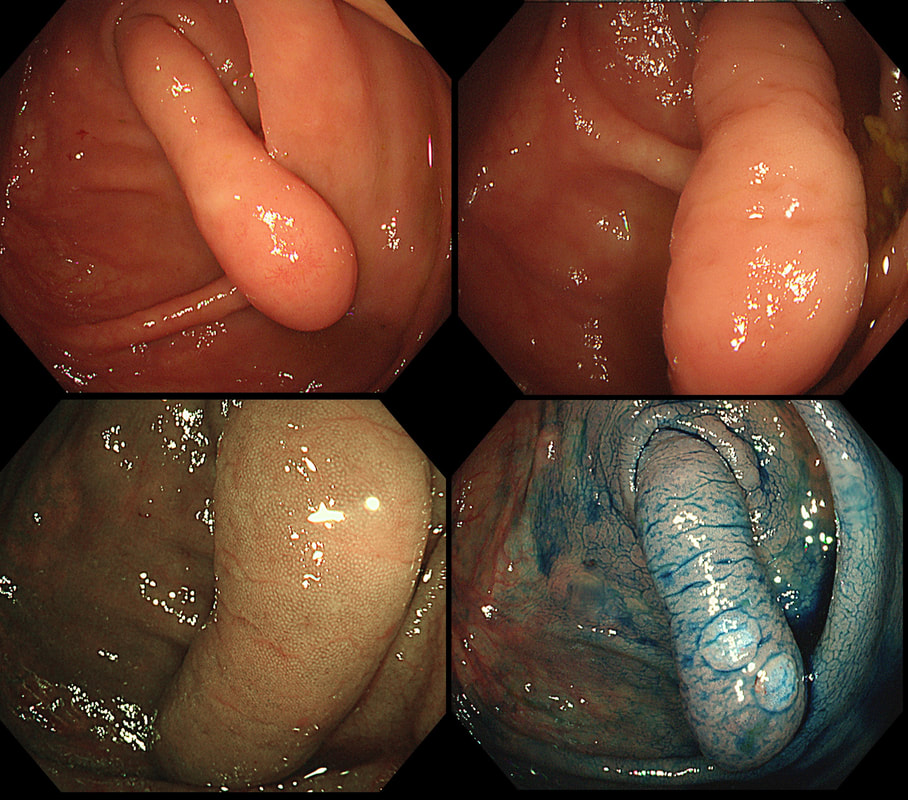
Just a bit of fun! Above are four types of benign polyps which can be found in the stomach, duodenum and colon respectively. I've used a 'plugin' which will hopefully make it easier to see the polyps on a small screen. BUT WHAT ARE THESE FOUR POLYPS ? A = B = C = D = You'll have to make up your mind and then click 'Explanation' below to reveal the correct answers ! EXPLANATION
The 3 polyps in column A are all adenomatous polyps. Flat and plaque-like in the stomach, pale in the duodenum and a sessile TVA in the colon. Column B shows NET's with the prominent vessels along it's side in the stomach and colon whilst the duodenal NET has the typical central depression. Column C shows 'hamartomatous' polyps seen in Peutz-Jeghers syndrome. There is hardly ever any dysplasia within these polyp and it's uncertain what the 'precursor lesion' is for these patients GI cancers Column D show inflammatory polyps which are typically angry red and sometimes with pretty white spots ! This patient has been referred for a dilatation WHAT IS THE AETIOLOGY OF THE STRICTURE? explanation
This short almost membrane-like stricture is of course a Schatzki ring, named after the German-American physician Dr Richard Schatzki. It's usually easy to treat these with a balloon dilatation. This particular case is unusual as two dilatations were required. However, rather than going ahead with a second dilatation to 20mm (our largest balloon in Leeds), I decided to cut the membrane with the tip of a snare and the diathermy set on the normal sphincterotomy setting.
The uploaded video is a good example of this mishap when cutting across yourself. I don't think that I perforated the full thickness of the oesophagus but applied a clip just in case (I've never regretted placing too many clips). 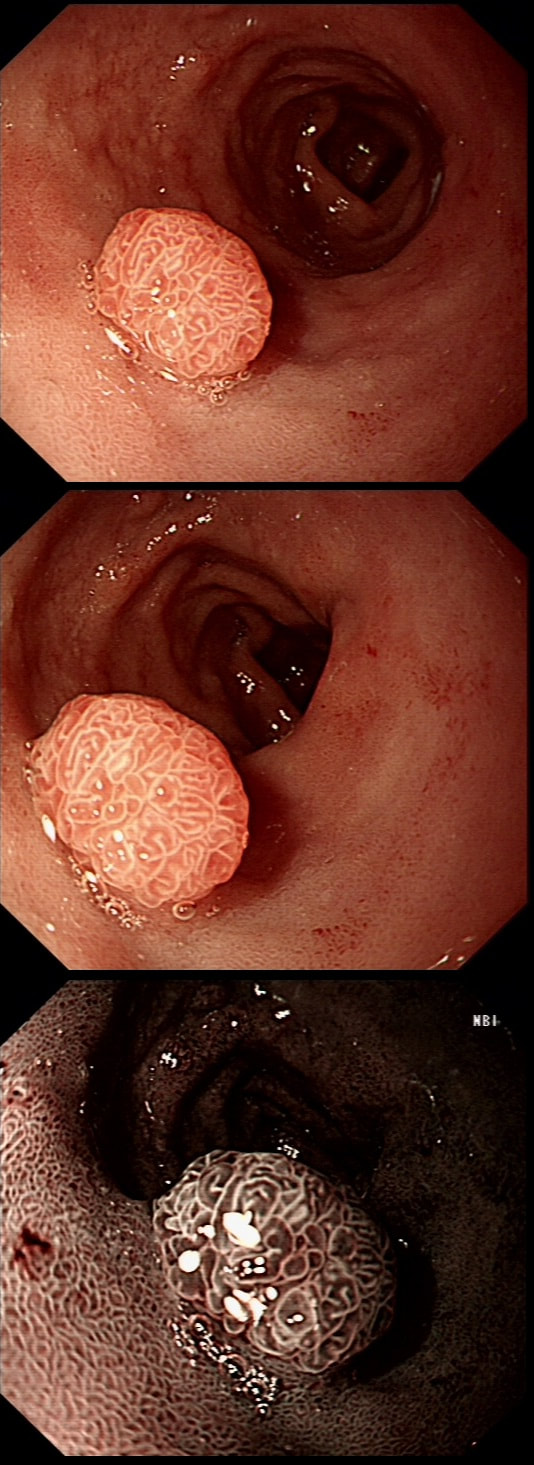
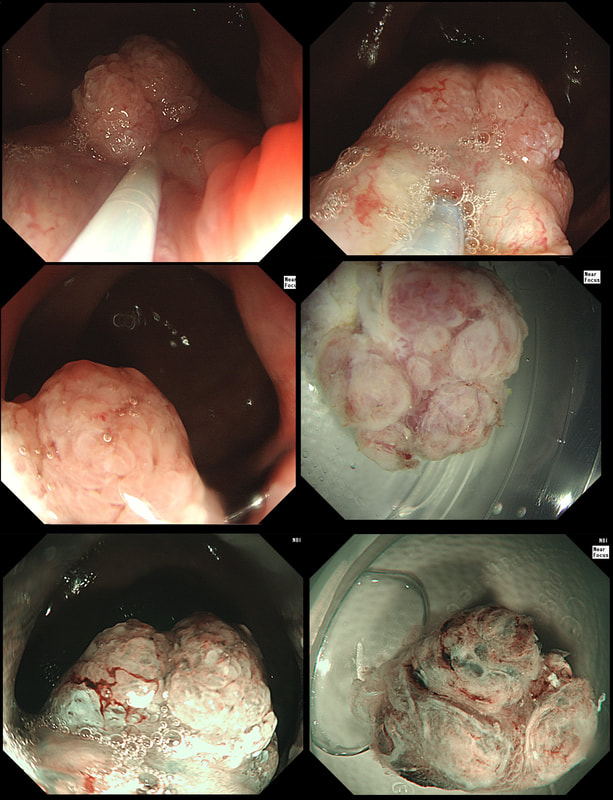
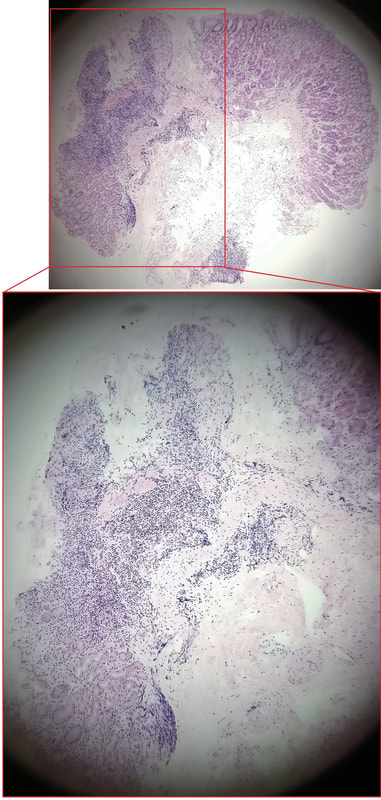
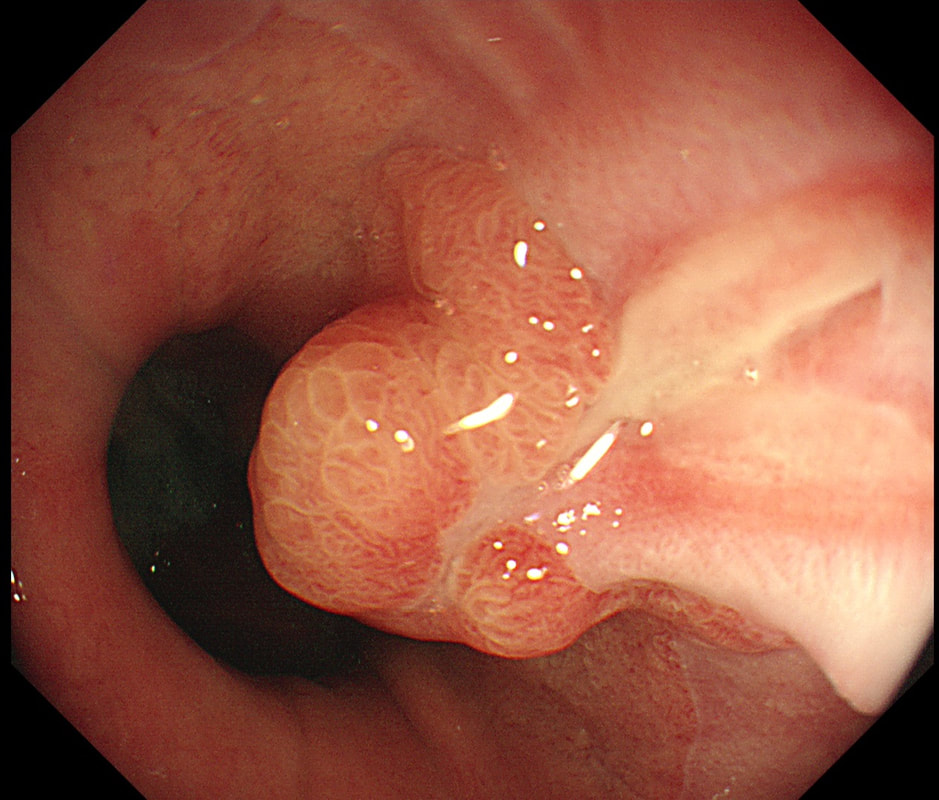
A rather beautiful polyp found in the duodenum of a patient undergoing upper GI surveillance
WHAT IS THE LIKELY HISTOLOGY?
explanation
This polyp doesn't look adenomatous. Remember that in the duodenum, the adenomatous polyp are usually flat, often with white white edges and with a slit-like or gyrate crypt pattern. Of course, in this case the crypt pattern is gyrate, almost exaggerated gyrate! The rather beautiful surface rules out an inflammatory polyp and an NET, both of which don't have this pretty surface structure. Even the histology is rather beautiful, see example below!
In addition, as you probably know, most duodenal NET's will have a central indentation and will not have a distinct crypt pattern. Cutting to the chase, this patient has Peutz-Jeghers syndrome ! This is a good example of the hamartomatous polyps these patients develop throughout their GI tract. Similar hamartomatous polyps also develop in the 'Cronkhite-Canada syndrome and Juvenile polyposis. Hamartomatous polyps are characterized by 'disorganized overgrowth' of the normal tissue but without visible cellular instability (dysplasia). Of course, these patient have an appalling lifetime risk of developing cancer which can be as high as 90%, including gastric, colorectal, breast, colorectal, and pancreatic malignancies. Unfortunately, there is no no evidence that removing hamartomatous polyp will reduce the subsequent risk of cancer. For this reason the only justification for attempting the somewhat hazardous endeavour to remove PJS polyps deep within the small bowel is to reduce the risk of subsequent intussusception. Rather surprisingly, a quick medline search has not revealed any RCT evidence that this actually is worthwhile ! 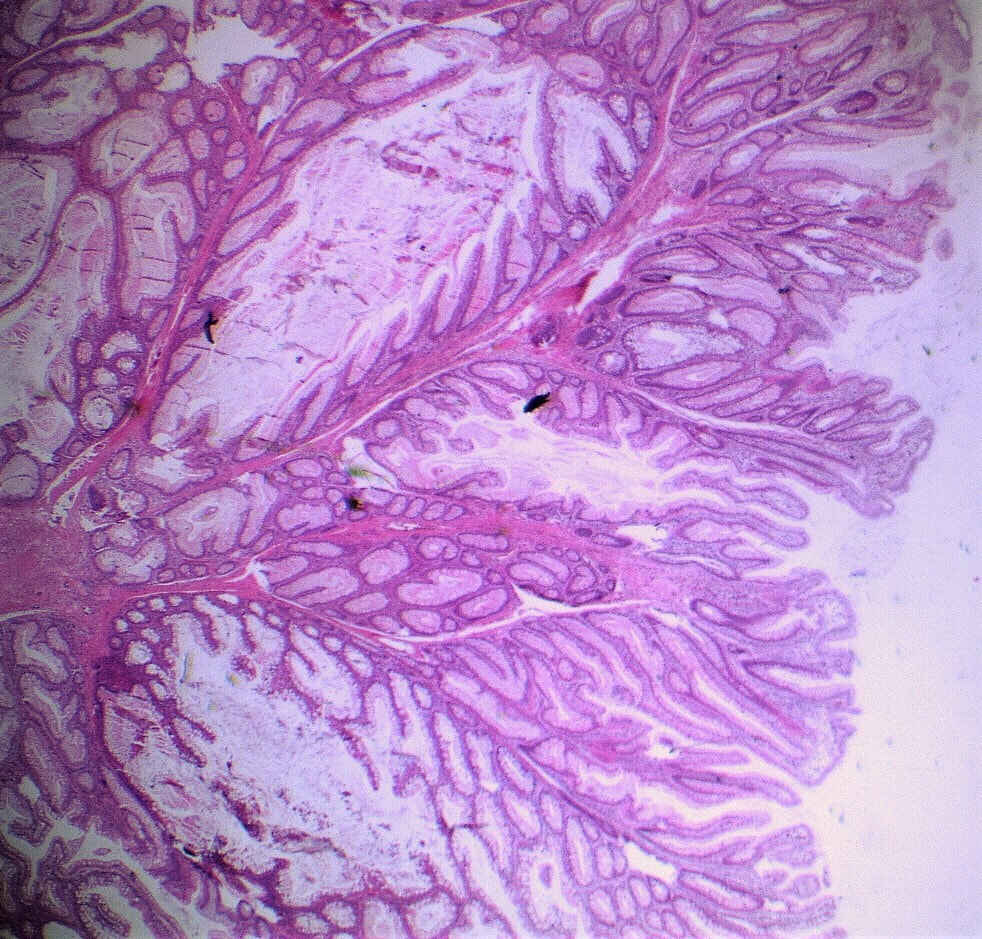
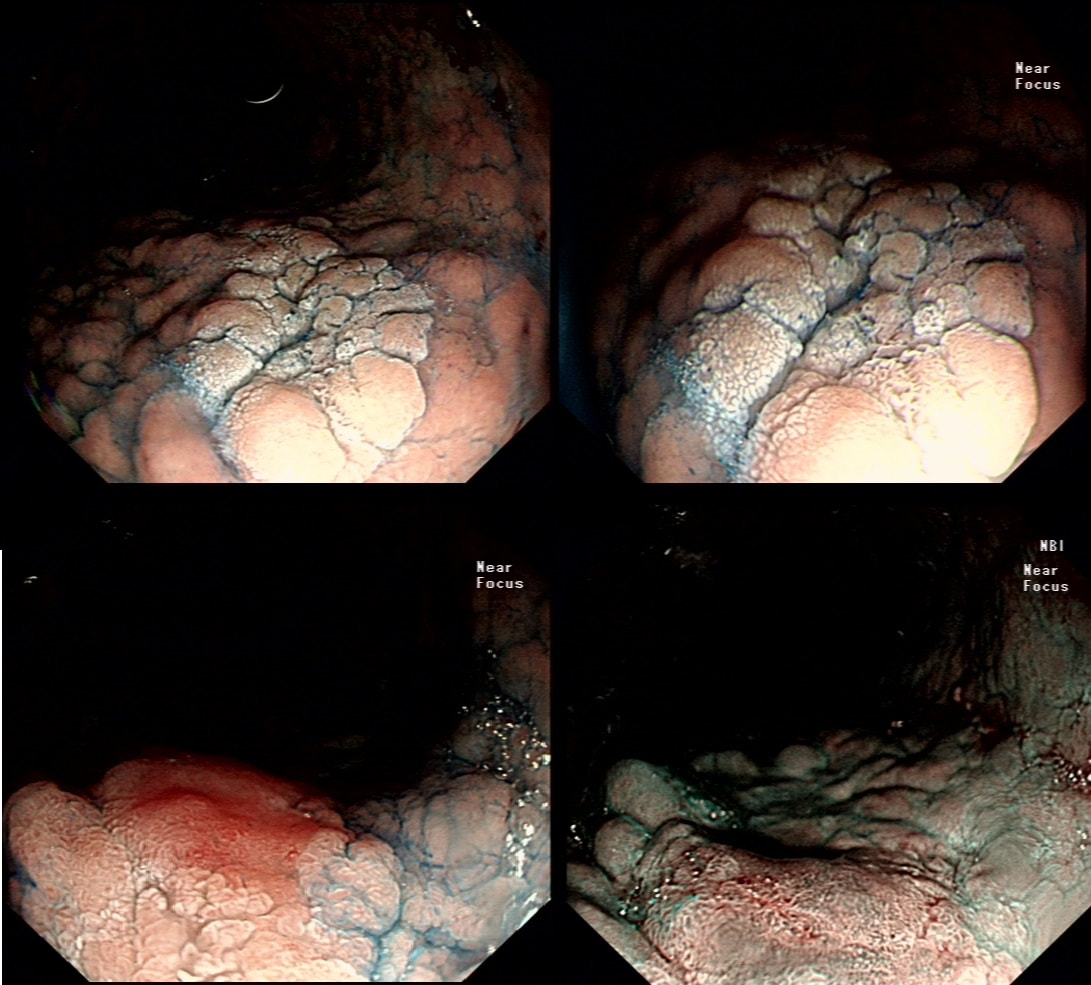
These are the NBI images of a young woman complaining of chest pain, dysphagia and reflux symptoms. She also complains of feeling of a 'lump at the back of her throat'.
WHAT WAS THE ORIGINAL DIAGNOSIS?
explanation
This patient was found to have a large oesophageal inlet patch at the index endoscopy a year ago. Although his symptoms were rather mixed, we have spent 4 sessions on ablating her inlet patch with APC.
Of course, how often you find these will depend on whether you use NBI/FICE/BLE during extubation. Of course you should do because you are then less likely to miss squamous dysplasia! An interesting study reported that gastric inlet patches contained glucagon cells which would normally only be found in the embryo and subsequently disappear. To remind you, the hormone glucagon is normally produced by the alpha cells of the pancreas! Glucagon-like peptide-1 is also secreted by some cells in the ileum and colon. Anyway, the implication is that the gastric inlet mucosa is actually an embryonic left-over. Interestingly, there appears to be a lower prevalence reported in older populations, and some authors suggest that inlet patches may regress with age! Seems odd for a congenital condition? Endoscopic studies have found inlet patches in up to 10% of patients. Whether these give rise to any symptoms is contentious. It has been suggested that inlet patches may give rise to globus sensation due to irritation of the upper oesophageal sphincter by acid or mucus. Furthermore, others have suggested that H. pylori colonization of the heterotopic gastric mucosa causes symptoms. Others believe that it's not just the upper oesophageal sphincter which is abnormal but the entire oesophageal motility may be disorganised in these patients. However, prospective studies have usually not found that patients in whom an inlet patch is found, present with any different symptoms compared to patient without an inlet patch. Of course as anywhere in the body, cancer may develop. A study in Digestive Diseases & Sciences [2018;63(2):452-65] reported on 156,236 gastroscopies and may have found 3 cases of malignant conversion. Assuming that 10% of their patients had an inlet patch, that would suggest that you would have to regularly surveil 500 patients with an inlet patch over many years detect 1 cancer. If you grab 500 random people off a street and scope them annually for 5 years, wouldn't you pick up more than a single early oesophageal cancer? Seems like that lemon is not worth the squeeze? Finally, how about our patient? Over the period of one year, we spent about one hour ablating and completely getting rid of that large inlet patch (well two inlet patches really). The patient reported that symptoms were much better for a couple of months but then returned as before. Of course as she no longer has an inlet patch, we can now conclude that it never did contribute to her symptoms. Must admit that I was sceptical from the start! Show me a prospective RCT with evidence that ablation provides a clinically significant improvement in patients globus symptoms for more than a few months! Until I see that RCT, I will not be offering ablation for these patients. 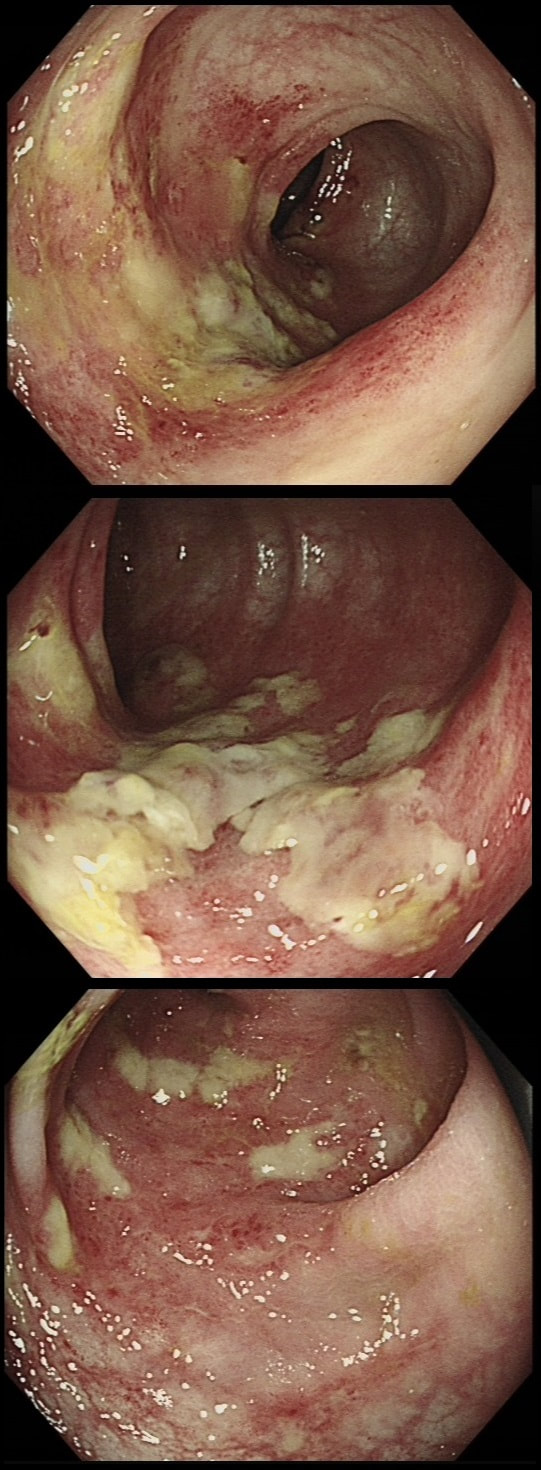
This 70 year old patient with known ischaemic heart disease presents with sudden onset bloody diarrhoea. He undergoes a flexible sigmoidoscopy the following morning and this is what the sigmoid colon looks like. With support and conservative measures symptoms subside and the patient is discharged a week later. However, a week later the patient presents again. Now with hypotension, abdominal distention, fever and a raised white count. An abdominal X-ray is done on admission (below).

WHAT IS THE LIKELY DIAGNOSIS?
explanation
There is little mystery that the first presentation was due to ischaemic colitis. The second presentation is more tricky. He actually presented with an ileus and pain this time. Actually, the patient had been on aspirin but this had been stopped at the previous admission. This was clearly a mistake as the second presentation turned out also to be due to ischaemic colitis. This time the ischaemic colitis was more severe but he did recover in the end.
After ischaemic colitis about 10% of patients develop and ischaemic stricture but it takes longer than a single week to develop. The hallmark of an ischaemic colitis are areas of longitudinal ulceration, on the anti-mesenteric border (90° to any diverticulum) where the blood flow is the slowest. Of course, endoscopically its difficult to tell where the omental reflection is situated. However, the ulceration will run along one aspect of the colonic circumference. Of course in the epicentre of the ischaemic (typically around the splenic flexure), the ulceration may well be circumferential. Ischaemic colitis is surprisingly easy to confirm histologically as the pathologists look for crypt withering and fibrosis. By the way, if the mucosa looks dusky and there is no bleeding on taking samples, the likelihood is that the colon is turning gangrenous, associated with a >50% mortality rate. 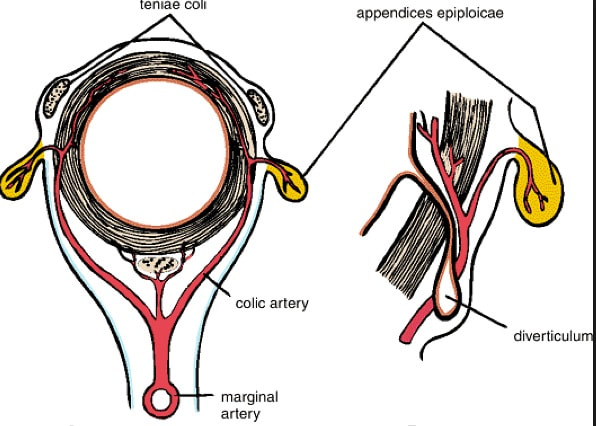
A very odd looking polyp at the anal verge. I removed it but still couldn't really make out what it was!?
WHAT IS YOUR BEST GUESS AT THE MOST LIKELY DIAGNOSIS?
explanation
This is rare stuff! I was clueless although reassured that the thing was soft and didn't feel malignant when squeezed between my fingers.
It proved to be a (rare) 'cloacogenic polyp'! You'd be excused if you have never heard of this (I hadn't). Apparently these were first described as recently as 1981! The same year that I was born ☺! Essentially they are inflammatory polyps arising from the transitional zone of the anorectal junction. They can be much larger than this and even be multiple and can occur at any age. Patients are usually asymptomatic but could (naturally) present with some blood on the toilet paper (this patients complaint). Histology is similar to that of solitary rectal ulcers with inflammation and fibromuscular hypertrophy. For this reason it is perhaps not surprising that they are linked with constipation and straining. Rare associations include small nearby cancers and human papillomavirus infection. This lesion was found in the ascending colon. WHAT IS THE MOST LIKELY DIAGNOSIS? explanation
The apparent lesion is covered with a normal layer of mucosa. In addition, it seems very soft. However, the lesion looks more translucent than yellow! Of course, it's another lymphangioectatic cyst ! Naturally, you confirm this by giving it a prod with your biopsy forceps. If soft, its either a lipoma or a cyst. If firm, it's either a GIST, leiomyoma or a metastasis (I guess). 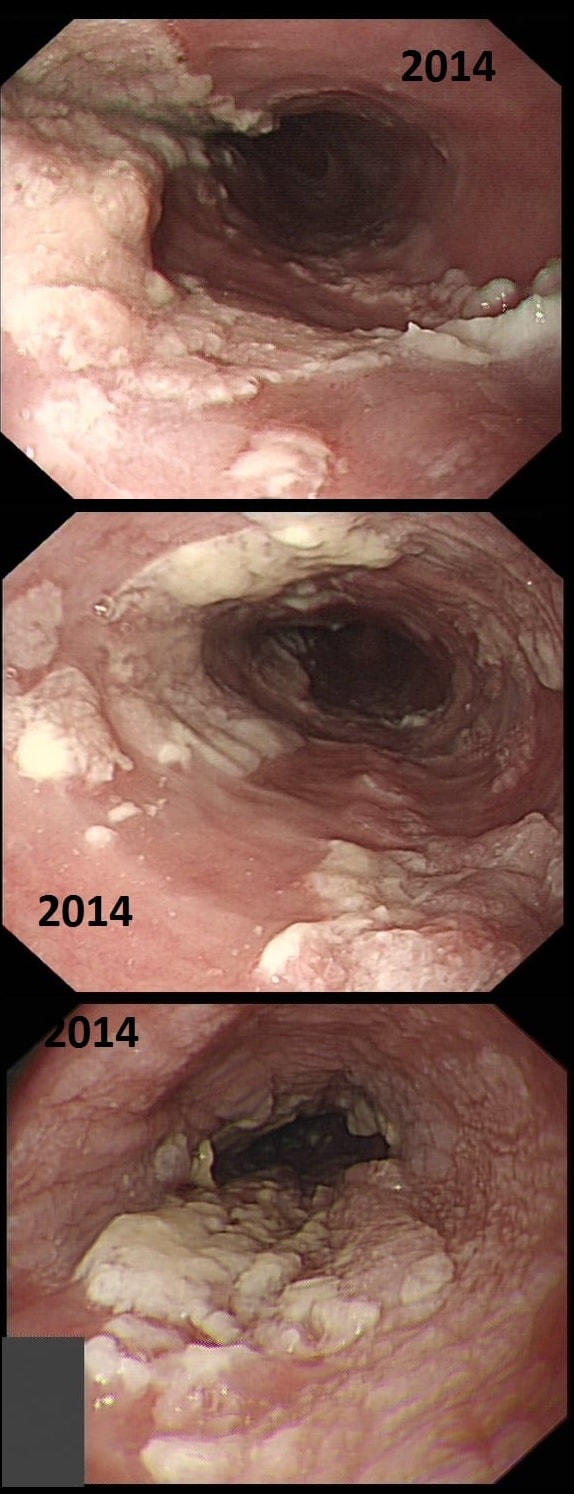
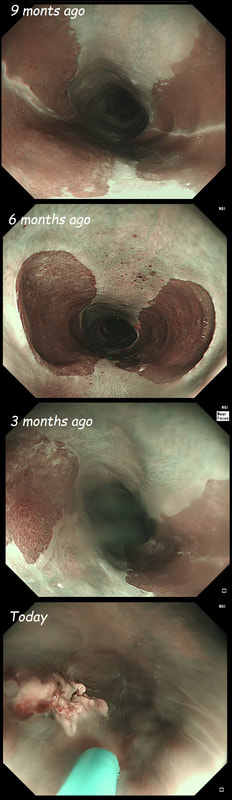
This patient presented with odynophagia and this is the appearance of the oesophagus from 2014
WHAT WAS THE INITIAL DIAGNOSIS IN 2014 ?
explanation
This is a case from Pradeep Mundre at Bradford. The correct diagnosis was 'Diffuse oesophageal Squamous papillomatosis'. Unfortunately, by 2021 the patient re-presented with worsening symptoms was was found to have developed a 'basaloid squamous cell carcinoma' (photo below).
Squamous Papillomas and Squamous papillomatosis of oesophagus Papillomas are finger-like projections that histologically have a central fibrovascular core surrounded by proliferative squamous epithelium with keratin outside this. Of course these are usually small and isolated. However they can become larger and rarely there is diffuse changes as in this case, and term 'oesophageal papillomatosis' is applied. There is little in the published literature on oesophageal papillomas with just a few published case series. Aetiology is unclear as to why some grow large whilst the vast majority remain tiny. Published literature has been conflicting with regards to association of oesophageal papillomas with HPV infection. Clinical relevance, natural history and whether this is a premalignant lesion, remain a matter of debate. There has been a few case reports of progression/ association with squamous cell carcinoma, especially with diffuse squamous papillomatosis. In other organs, the causal link between human papillomavirus infection and cervical, anogenital, and some oropharyngeal malignancies has been established by both molecular and epidemiological data. Management Owing to paucity of evidence, it is unclear how to manage this. I guess we can translate knowledge from other areas and use this in oesophagus Isolated small papillomas are easy to ablate with a quick 'zap' of APC. For larger areas of more diffuse papillomatosis, ablative techniques, such as APC ablation or cryoablation or radiofrequency ablation may all be considered. However biopsies or even EMR may be prudent of more 'chunky' areas to rule out possibility of 'prevalent' dysplasia/malignancy. Bjorn has treated a couple of patients with very large areas of oesophageal squamous papillomatosis with APC ablation. Of course, it's quite daunting when you start and it takes a special patient not to freak out when belching up the fumes of vaporised mucosa (a GA would make it easier for the patient of course). However, these lesions actually turn out to be easy to ablate and you will be surprised at the progress when the patient returns for a re-check (usually about 3 months later). However, most patients will probably require 3-4 sessions when the surface area involved is extensive as in this case. Of course, it's difficult to give a general advice about management. Clearly the risk of an elderly patient living long enough to develop a SCC must be small. Conversely, in a young patient, ablation to try to clear the oesophagus will avoid the need for surveillance and is probably justified. Reference Alomari et al Successful Treatment of Extensive oesophageal Squamous Papillomatosis With Cryotherapy, ACG Case Reports Journal: March 2019 - Volume 6 - Issue 3 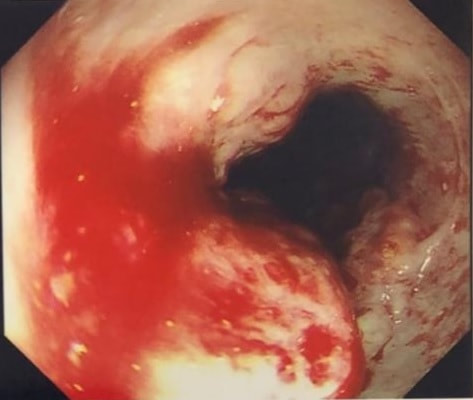

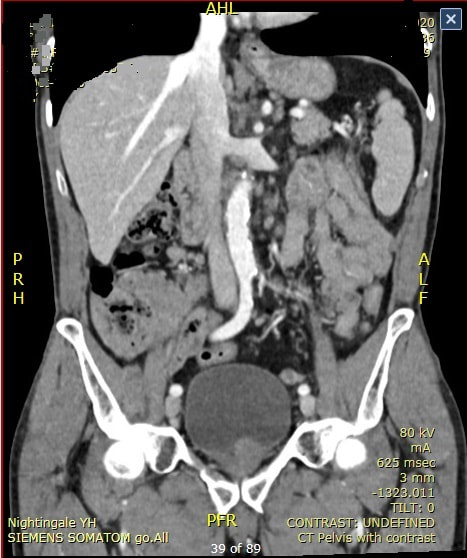
A 65-year-old man presents with a 1-week history of a worsening low abdominal pain. The abdominal pain was preceded by exertional chest pain that settled with anti-anginal therapy prescribed by the patient’s GP.
Apart from hypertension that is managed with ramipril, the recently started anti-anginal drug nicorandil and low-dose aspirin, the patient is well and able walk several miles without shortness of breath. Routine blood tests are normal on admission and the patient denies taking an NSAID or paracetamol. After the CT above and colonoscopy is carried out showing the above caecal inflammation. Unfortunately, the patient soon deteriorates requires an emergency right hemi-colectomy before histology is to hand. WHAT IS THE MOST LIKELY DIAGNOSIS?
explanation
Getting this diagnosis wrong would have profound implications for the patient ! The ulceration would be likely to recur and the patient may even present with further ulceration unless it is recognised that the cause is his nicorandil tablets !
Nicorandil, a combined venous and arterial vasodilator is effectively the drug of last resort for angina. The reason is that there have been numerous reports of ulceration affecting skin, eyes or mucous membranes which have accumulated since the drug was launched in 1994. Small aphthous ulcers are said to occur in up to 5% of patients but more severe, painful and deep ulceration may ensue. In the gastrointestinal tract, perforations, fistula formation and abscesses are recognised complications. Patients taking NSAID’s, steroids or have diverticular disease are at particular risk. There is also some evidence that the risk of ulceration increases with dose and ulceration may be precipitated by an increase in dose. The underlying mechanism by which the drug causes ulceration is unknown. However, nicorandil-induced ulcers persist until the drug is withdrawn although healing may take up to 6 months. In addition to patients with a history of ulceration of mucosal membranes, nicorandil is contraindicated in patients with hypokalaemia, heart failure and renal impairment. 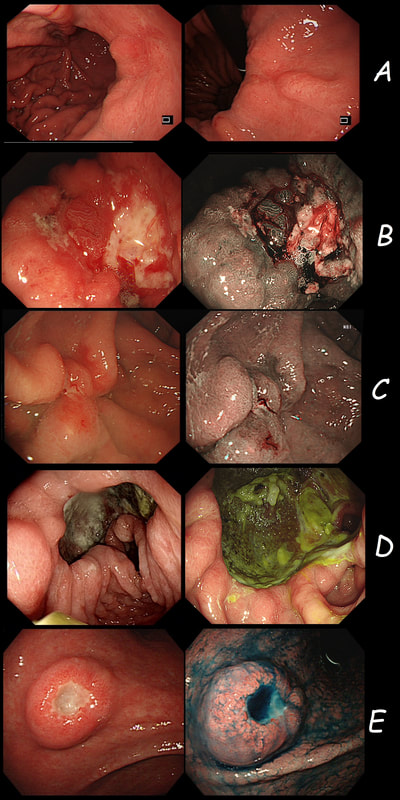
Just a bit of fun! Five 'gastric ulcers', three of which are malignant.
WHICH 3 ULCERS ARE CANCEROUS?
explanation
Image A is a diffuse type gastric adenocarcinoma, which is strictly speaking not an ulcer (they rarely ulcerate of course). These are notoriously difficult to pick up and only show up as either a tiny pale submucosal spot, a red patch as in this case or as a more extensive patch of inflamed gastric mucosa.
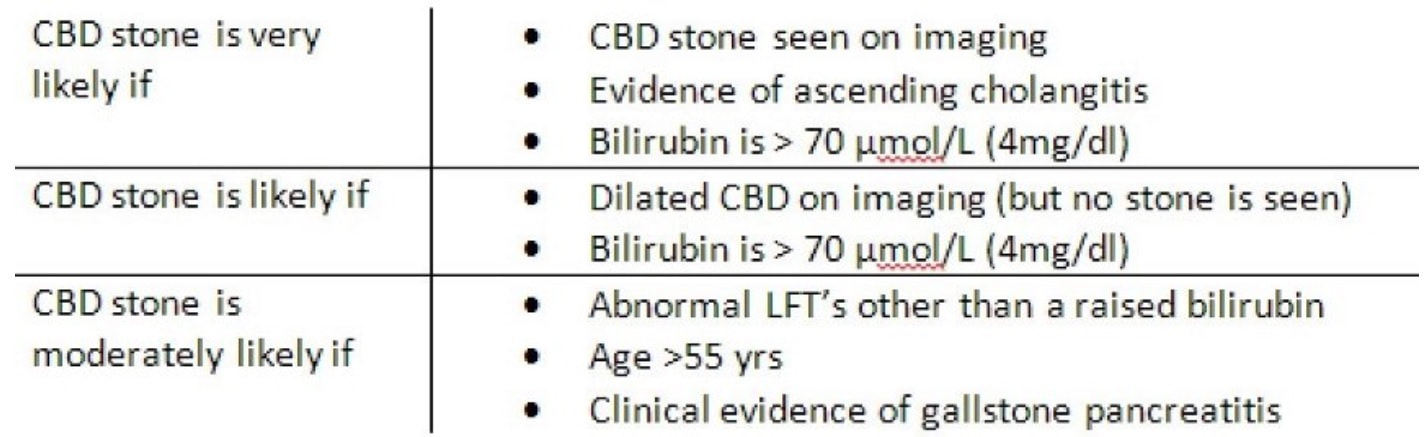
Image B was a T2 gastric cancer in which initial biopsies had been entirely benign, only reporting 'reactive atypia'. However, endoscopically there is a rim of thickened, red indurated mucosa surrounding the ulcer. Image C is an early gastric cancer pulling on the nearby gastric folds. It was removed endoscopically and turned out to be intramucosal only. Image D is of an entirely benign 'giant' gastric ulcer. ‘Giant gastric ulcers’ are (arbitrarily) what we call ulcers which are ≥3cm in size. In our Leeds series of 111 ulcers, 42 were malignant (34 adenocarcinomas and 5 lymphomas as well 3 rare tumours). In our series, logistic regression revealed that the (predictable) predictors for malignancy were; 1) increasing patient age, 2) larger size of giant the gastric ulcer and 3) the endoscopist making a diagnosis of a likely malignant ulcer. Finally E is an ulcerated fibroid polyp and not an ulcerated GIST! Of course you can't tell the two apart on endoscopic grounds! A middle aged patient presents with obstructive jaundice. There is a history of upper abdominal pain for 2 months and jaundice for about 4 weeks. She has also lost some weight loss and had night sweats. On examination she is apyrexial, obviously jaundiced and slightly tender in the epigastrium Hb 98 MCV 71 WCC 4.17 Plat 338 CRP <5 (<10) Amylase 102 (<110) Bili 75 µmol/L ALT 910 iu/L ALP 302 iu/L Albumin 37 g/L INR 1.0 An abdominal ultrasound is carried out (images below) 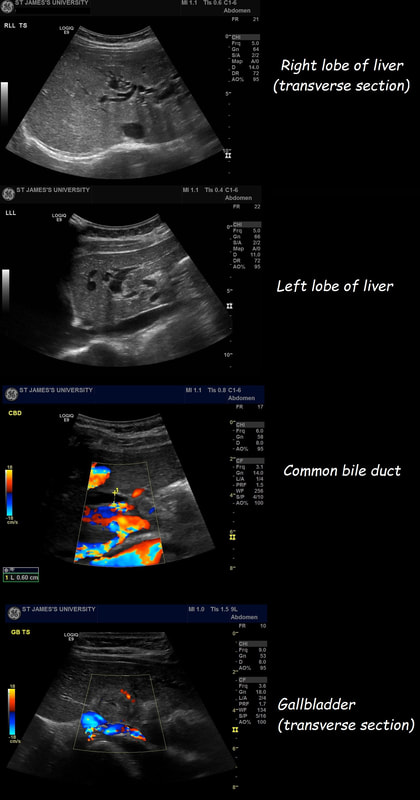 If you work outside of the UK, and actually do abdominal ultrasound examinations you will be able to see that the gallbladder is extremely thick walled and hyperaemic. There is also intrahepatic biliary duct dilatation but the CBD is of normal calibre (6mm) and no stones can be seen. I haven't included the images showing that the pancreas, pancreatic duct, liver, abdominal aorta, spleen and kidneys were all normal. WHAT IS YOUR CLINICAL DIAGNOSIS? explanation of the case (so far - there is more to follow!!! )
Choledocholithiasis should be your clinical diagnosis at this point. This is because the ‘strong likelihood criteria’ are fulfilled as follows;
To search further for gallstones, a CT scan was then requested (below).  You can probably tell from the CT that The gallbladder is confirmed as thickened with some extrinsic compression of the bile duct at the porta hepatis to explain the intrahepatic ductal dilatation already seen on ultrasound. The distal bile duct is confirmed as collapsed with normal appearance of the pancreas, kidneys, adrenal glands and spleen. WHAT IS NOW THE DIAGNOSIS? second explanatation (and yes there are further developments around the corner)
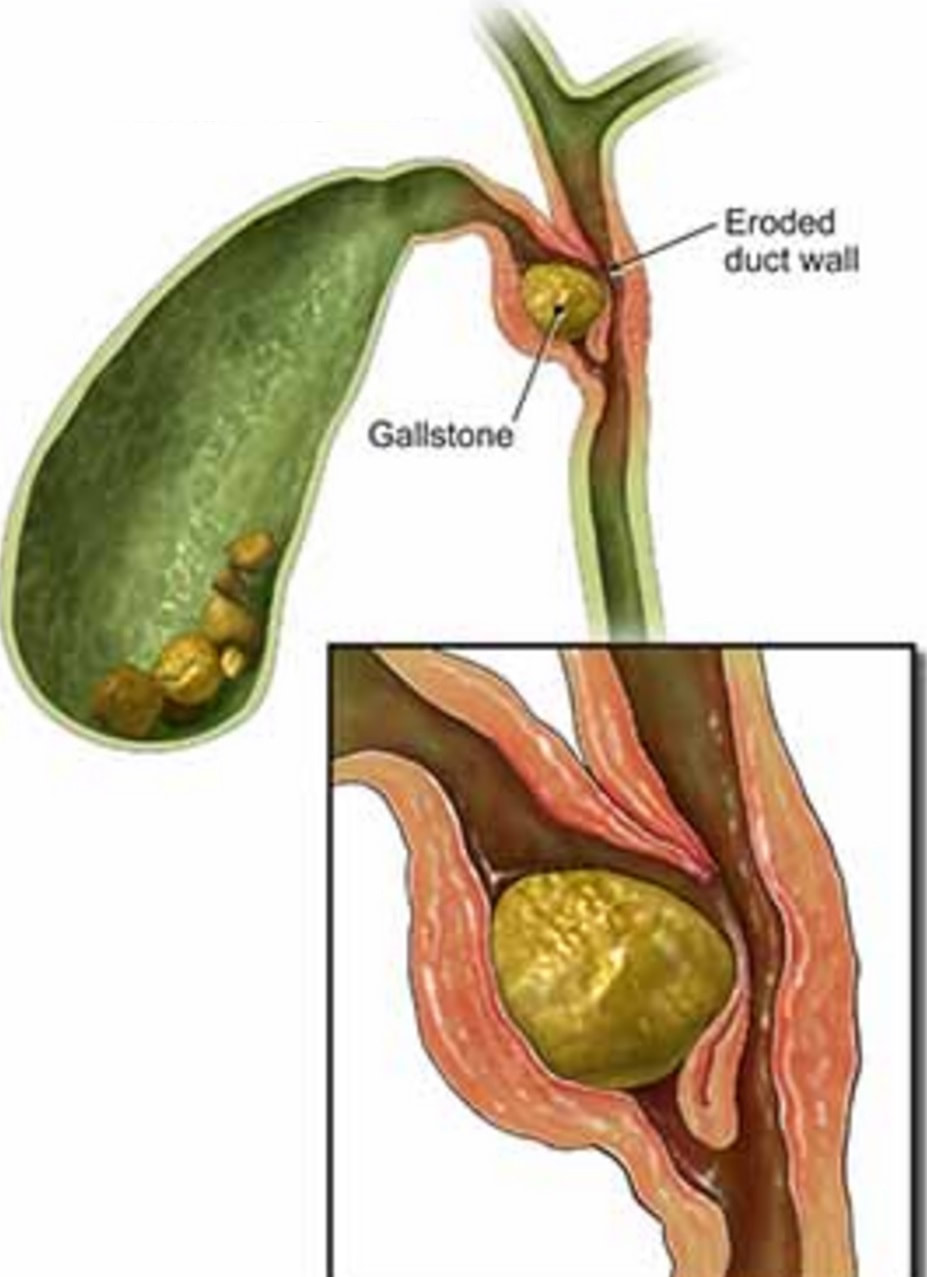
The CT report essentially describes a Mirizzi syndrome type 1. Pablo Mirizzi was an Argentinian Surgeon who first described the obstruction of the common hepatic duct (CHD) by an impacted stone in the cystic duct or Hartmann's pouch of the gallbladder. In Mirizzi syndrome type I there is no fistula between the gallbladder and CHD whilst type II-IV have a fistulous communication. Of course its difficult to tell on imaging if there is a fistula. For this reason the subtype of the Mirizzi syndrome is usually something discovered at surgery.
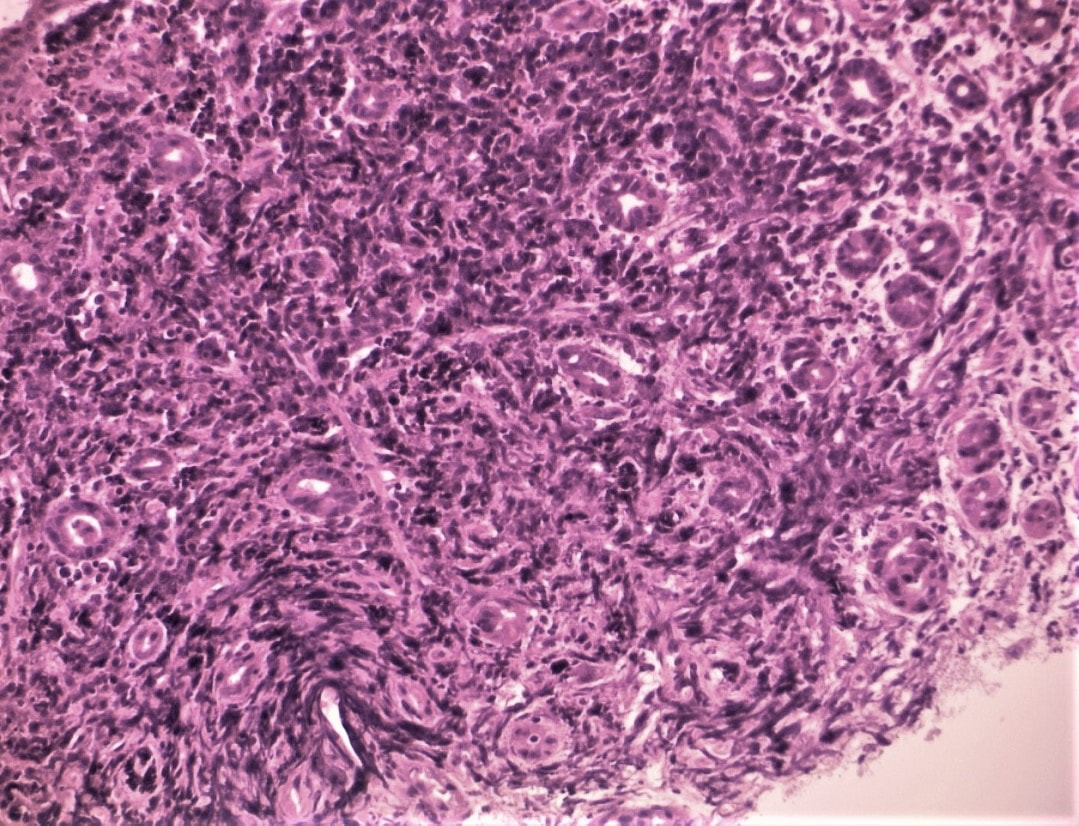
The patient does undergo a laparoscopic cholecystectomy but to the surgeons surprise there are no stones found within the thickened gallbladder or within the bile ducts. The gallbladder is analysed and the pathologists report that the: “Gallbladder measures 52 x 30 x 20 mm. The serosa is congested and wall thickness is 3 mm. No stone and no focal lesions. There is subacute cholecystitis with myofibroblastic proliferation of the wall and mild acute on chronic inflammation” Strangely enough, the jaundice does not resolve after surgery and for this reason an MRI scan is carried out which confirms a stricture at the common hepatic duct with mild intrahepatic ductal dilatation. At this point we decide to carry out an ERCP to sample the stricture and place a stent. Now you have all the pieces in this jigsaw and should know what's going on! WHAT DID WE MISS? FINAL EXPLANATION
Thanks for sticking with this case until the end! Actually, you did have an opportunity of getting the diagnosis when you heard that the gallbladder histology showed; "markedly thickened wall but with only mild inflammation of the gallbladder mucosa" ...
Of course, this doesn't make any sense! In acute cholecystitis there should be an INTENSE inflammation of the mucosa. So why is the gallbladder wall grossly thickened? A second look into the deeper aspects of that thickened gallbladder wall led to a revelation ! The 'second look histology' reported a 'poorly differentiated diffuse type adenocarcinoma deep within the gallbladder wall with single and files of small neoplastic epithelial cells (histology slides below). The pathologists reported that the tumour did appear to be coming from outside the gallbladder. Of course in the video you should have noticed that the gastric antrum was abnormal, a little indurated and thickened. The samples taken from the gastric antrum confirmed the same diffusely infiltrating adenocarcinoma. Those with VERY sharp eyes, would have seen the antral thickening on the initial CT which wasn't commented upon by the radiologist! So what was the final diagnosis? A diffuse type gastric cancer invading into the gallbladder, cystic duct and hepatic duct ! 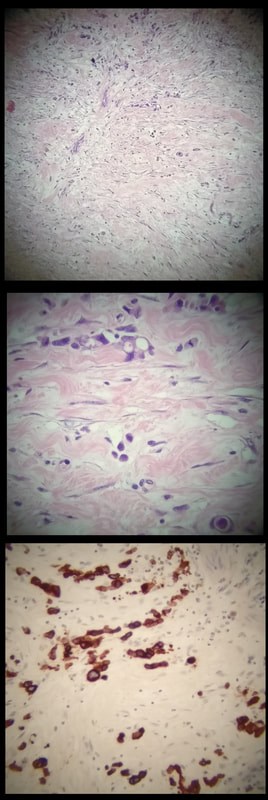
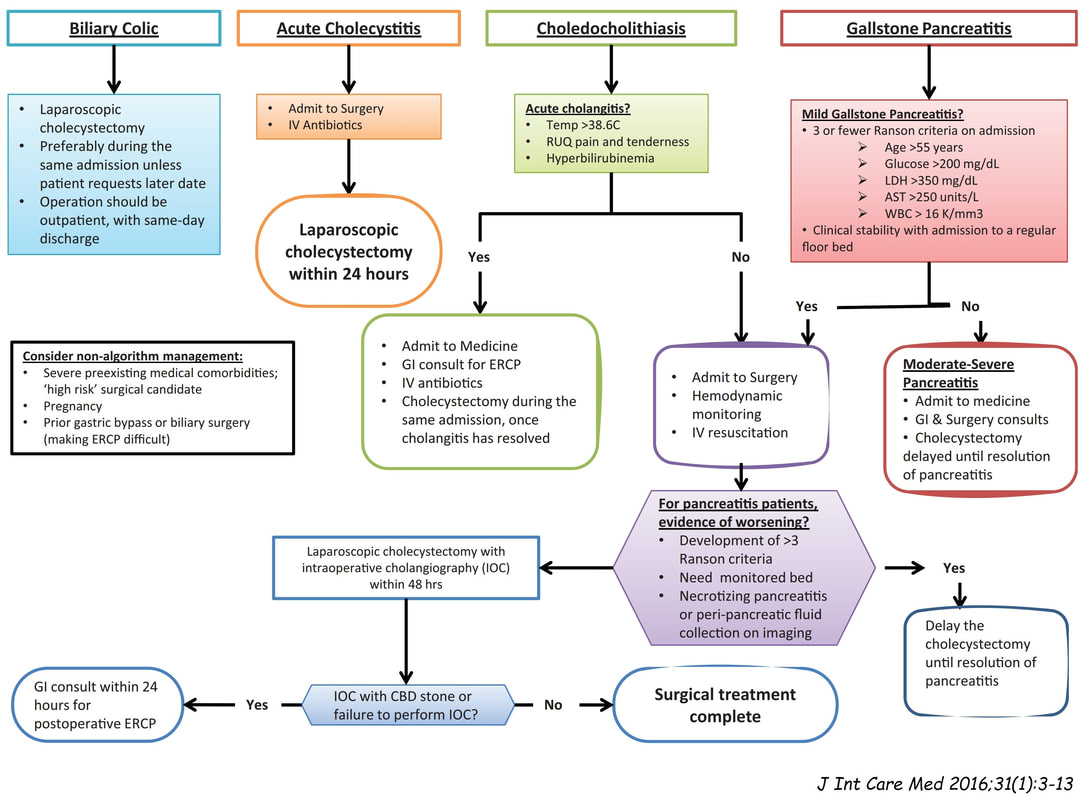
This may a good time to remind you of the management of gallstone related disease. The 'infographic' below from J Int Care Med 2016;31(1):3-13 summarises everything !
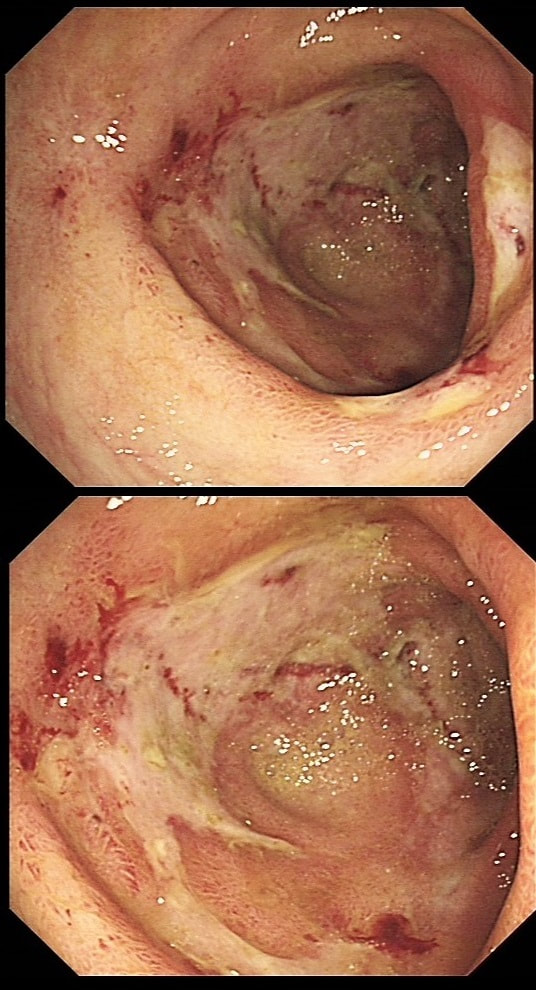
'Banding EMR of this junctional lesion is not going to plan! Biopsies had diagnosed IMca at least but both EUS and CT had been reassuring. WHAT WOULD YOU CONSIDER NEXT? explanation
Although EUS and CT had both been reassuring, this lesion is clearly tethered down to the oesophageal wall. The lesion is extending too deeply for endoscopic cure. Trying to 'push the boat out' by attempting removal by 'pull within the snare' technique or ESD will fail and will run the risk of perforation, potentially resulting in the upstaging of the lesion. Bail out ! I'm carrying out a dilatation (20mm) of a distal gastric stricture. WHAT IS THE LIKELY AETIOLOGY OF THE STRICTURE? explanation
The mucosa in the 4 o'clock position looks pale and atrophic. This is a 'scar' left after treatment of a gastric lymphoma. Of course, the scar would look the same following Hp eradication of a MALT lymphoma. However, this was after following chemoradiotherapy (CRT) for a 'Diffuse large B-cell lymphoma. Which is a far more nasty lymphoma and patients present with more advanced stage at diagnosis, and have a worse prognosis (about 75% of patients are alive at 5 yrs) than with a MALT lymphoma. This patient was treated with 6 cycles of R-CHOP chemotherapy and radiotherapy 30 Gy in 15 fractions. The risk of stricturing after gastric CRT is around 5%. My dilatations to 20mm didn't do much and the patient had to come back for a dilatation to 25mm before symptoms improved. 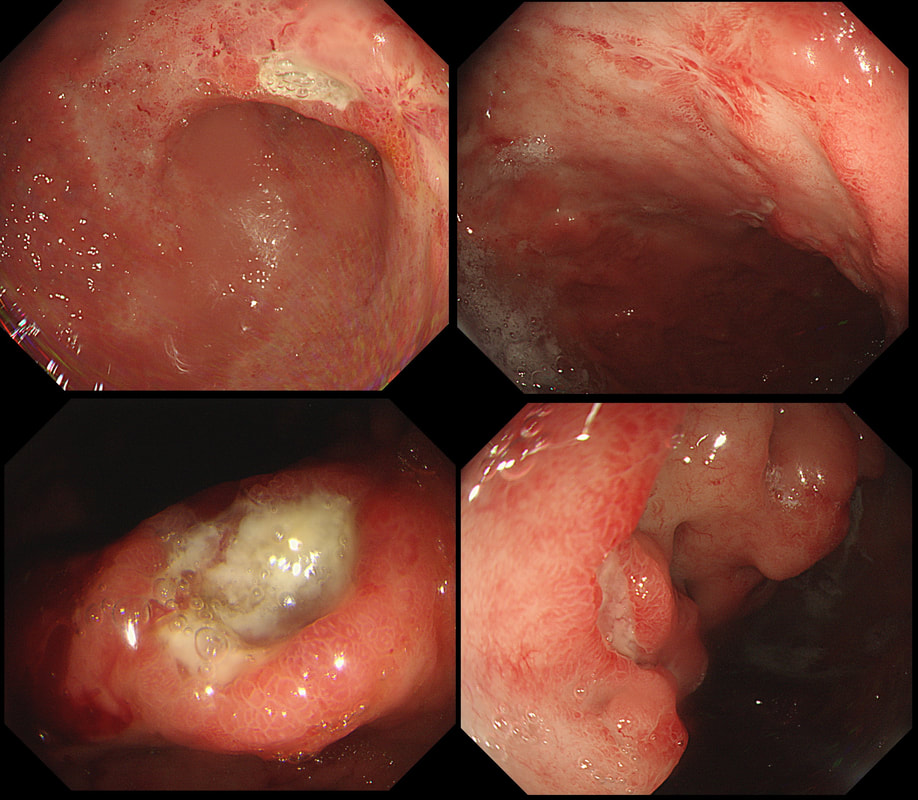
This ulcer was found on the lesser curve of a middle aged man with dyspepsia. Biopsies are taken and stained with H&E (below)
WHAT IS THE AETIOLOGY OF THAT GU?
EXPLANATION
There are only two possibilities here. Of course the ulcer itself doesn't tell you much. The mucosa surrounding the ulcer tells you more! With a benign ulcer, you would expect a thin rim of 'reactive' mucosa (looks red and a little villous). In the case of an intestinal type of adenocarcinoma a broad band of surrounding mucosa is red, indurated and thickened. In gastric lymphomas, the surface area of abnormal mucosa is usually far greater than the surface area of the ulceration. There are usually areas of atrophic and inflamed mucosa. Mucosa infiltrated by a diffuse type adenocarcinoma could look like this BUT it's unusual for it to ulcerate!
This patient has a MALT lymphoma ! Of course, I took samples for Helicobacters. Of course not every MALT lymphoma is linked with HP infection (about 2/3 cases are though). In this case our haematologists were optimistic of a good response to Hp eradication because all the 3 good prognostic criteria were met:
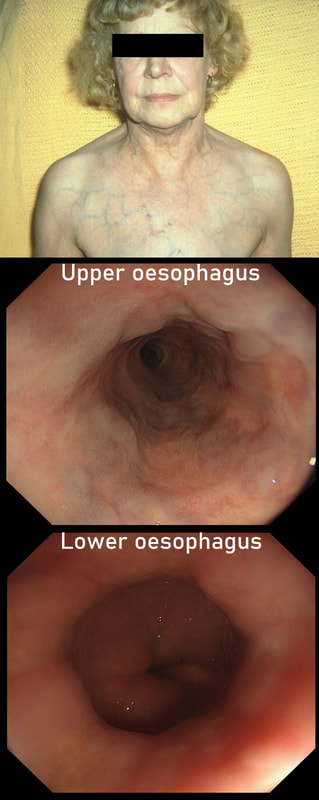
This lady is undergoing a gastroscopy
WHAT IS THE LIKELY DIAGNOSIS?
explanation
‘Downhill oesophageal varices’ are associated with superior vena cava (SVC) obstruction or obstruction or as in this particular endoscopic case, a clot in the right brachiocephalic, subclavian and axillary veins. I thought that just showing the oesophagus would make the question too difficult and therefore added the photo of a patient with SVC obstruction. Perhaps this made it too easy ☺!
Venous drainage of the oesophagus is through the azygos and hemiazygos veins (see below). When there is thrombus, retrograde flow pushes blood towards the heart via collateral channels. If the obstruction is above the level of the azygous vein, varices develop in the upper oesophagus. However, if the clot is below, or involves the azygous vein, varices will form along the entire oesophagus. Bleeding is rare as varices in the proximal oesophagus are situated deeper within the submucosa than distal varices. However, if you are asked to deal with bleeding, you need to place bands at the proximal end of the varix. Sclerotherapy is contraindicated in the high oesophagus because of the risk of spinal cord infarction and vertebral infarction. Glue injection should also be avoided as there has been a case report of a massive PE. 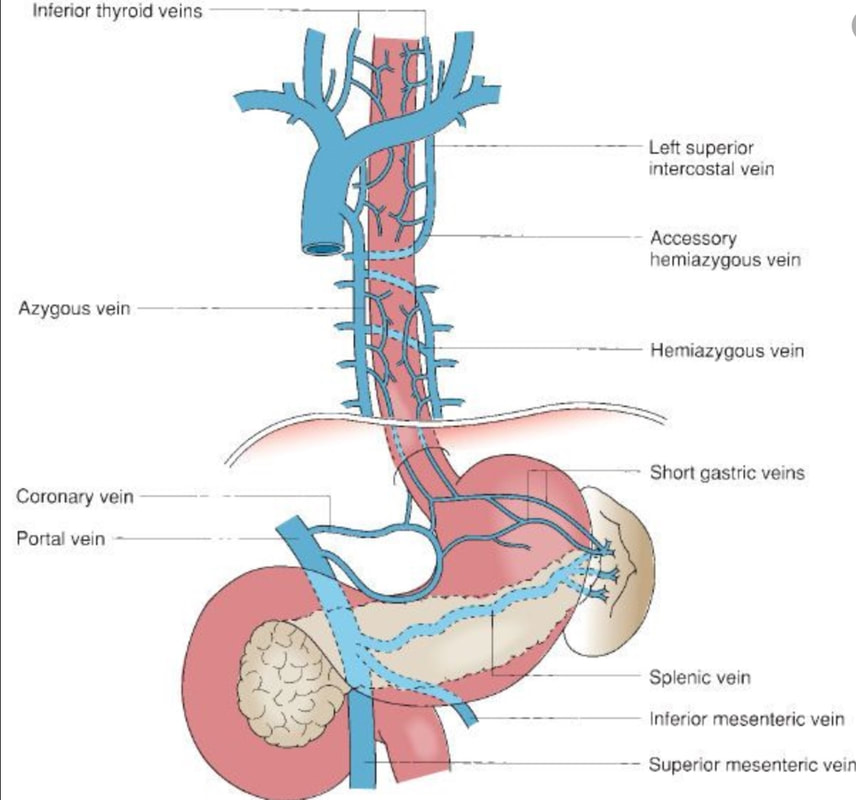
This patient was referred for an OGD after complaining of dyspepsia improving with PPI. This nodule is noted at the GOJ
WHAT IS THE MOST LIKELY DIAGNOSIS?
explanation
At first, that 'villous' surface may look disconcerting. However, you should know that in the oesophagus and stomach, polyps arising due to inflammation and oedema, (so called 'reactive or 'inflammatory' or 'hyperplastic' polyps) usually have a villous or gyrate surface pattern. In the stomach, these polyps often have an angrily red appearance and some white blobs making them look a little like pretty mushrooms (see example below).
OK, if this polyp is 'inflammatory', why is there inflammation? You can see a linear reflux ulcer in the 3 O'clock position. THIS is the reason for the inflammatory polyp. Of course, you'll take a couple of biopsies but as always, make an Endoscopic Diagnosis! You ARE a Professional and NOT a simple technitian unthinkingly feeding biopsies to the guys with brains! 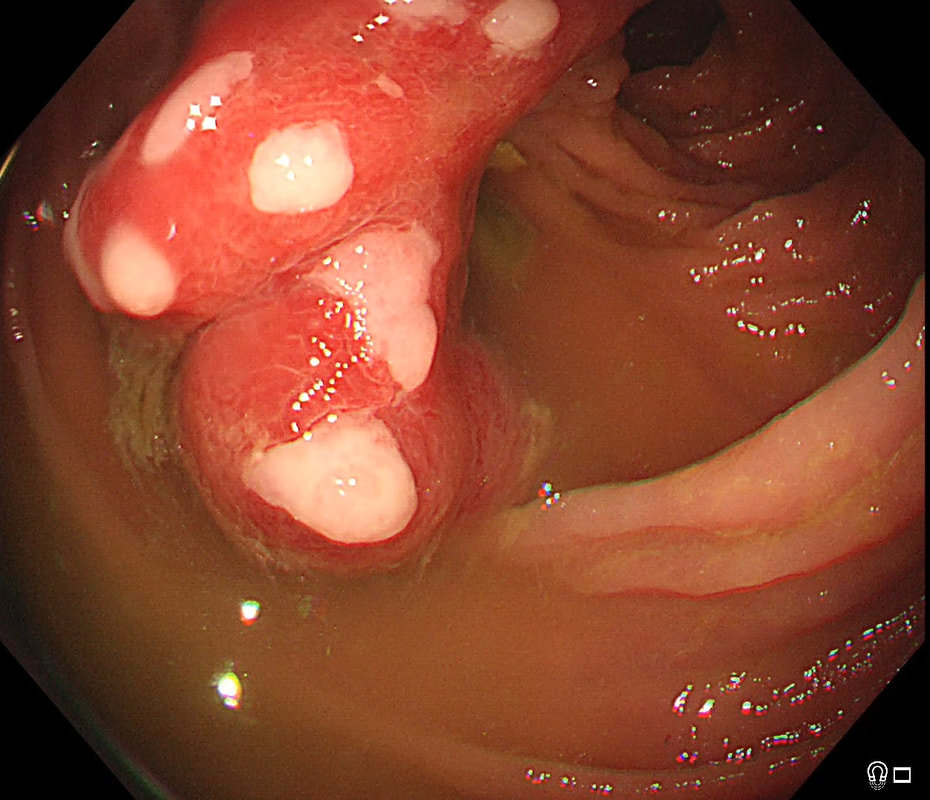
This was polyp found on the greater gastric curve.
WHAT IS THE LIKELY DIAGNOSIS?
explanation
Clearly there is a discrete nodule containing some small round crypt openings. If a dysplastic (mutated and genetically unstable) lesion produces a visible lesion, the pathologist calls it an 'adenoma'. Dysplasia in a flat mucosa is just called 'gastric dysplasia'. Of course in the colon there is a long established 'adenoma → carcinoma' sequence first proposed by Basil Morson a famous British pathologist. He estimated that about 2/3 colorectal cancer must be arising from an adenomatous precursor. What gives rise to the rest remained a disputed mystery until Jeremy Jass, another famous pathologists (and I really nice guy as I found, meeting him at a conference) proposed that serrated polyps may also give rise to cancer [Histopathology 2006;49:121-31]. His suggestion and data to support it, didn't really go anywhere for some 10 years but after he died in 2008 of glioma, the 'serrated pathway' to bowel cancer has become accepted.
Anyway, in the stomach things are even more complicated! There are at least 4 types of adenomas:
Of course, not every gastric polyp is adenomatous. Most are hyperplastic and look angrily red (because they have lots of capillaries) and often with white fibrin caps, making them look a little like mushrooms and may have a villiform surface reminisient of TVA's in the colon. Another common type are the 'Fundic gland polyps' which are full of cystic spaces and therefore look a little like frog-spawn. These usually develop in patients on PPI's but also in FAP. Polyps may also be hamartomatous as in 'Peutz-Jeghers syndrome', 'Cronkhite-Canada syndrome' and 'Juvenile polyposis'. By the way, the word 'Hamartomatous' implies that the polyp has arisen from overgrowth of multiple aberrant cell lineages rather than from a single, mutated precursor cell as in an adenoma. And then of course there are neuroendocrine tumours (NET's). A whole different thing which has a complete podcast dedicated to it. You can tell that a gastric polyp is a likely NET as they usually have little vessels crawling up it's sides. Finally, the lesion may be a gastric metastasis most commonly from breast, kidney, melanoma or HCC. By the way, there is a pitfall here as 'lobular breast cancer' mimics diffuse type gastric cancer. For this reason you should inform the pathologist if the patient has a history of breast cancer and you suspect a metastasis! 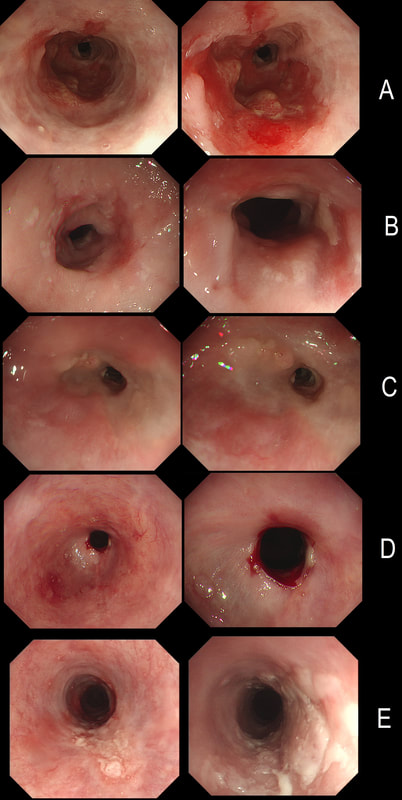
Here are 5 oesophageal strictures.
HOW MANY SHOW A CANCER?
explanation
Actually there are 2 cancers in there (case A and E). In order the aetiologies of the strictures are:
A = Adenocarcinoma B = Post radiotherapy stricture C = Peptic stricture D = Post ESD stricture E = Squamous cell carcinoma 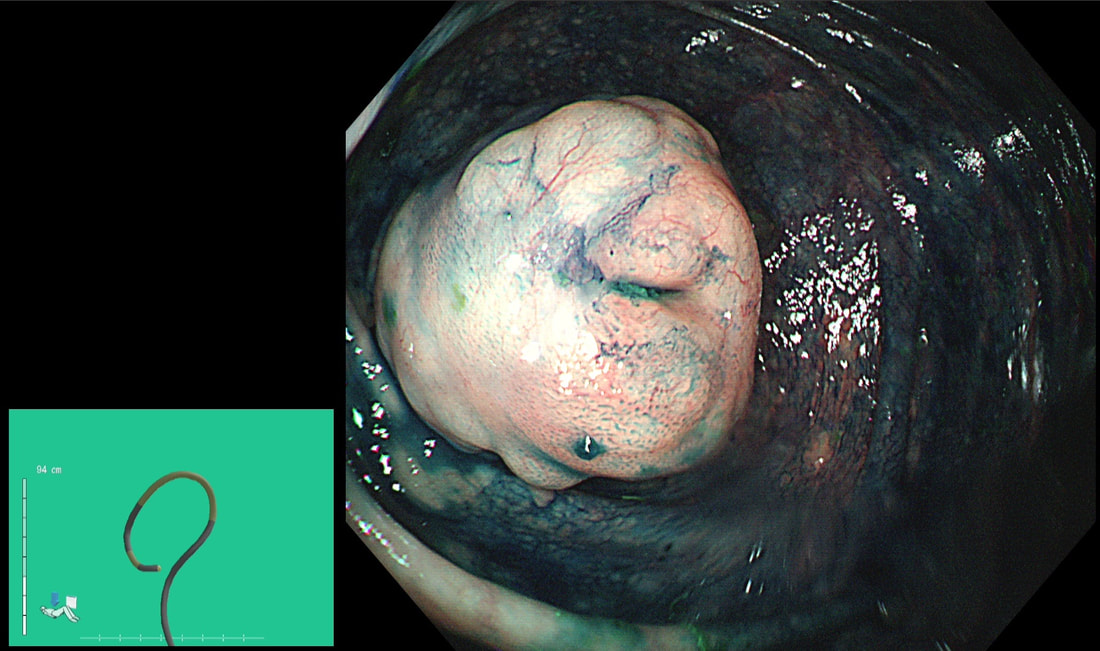
This polyp was found at the apex of the caecum. With some trepidation, a sample was obtained following which I requested the above CT
WHAT IS THE FINAL DIAGNOSIS ?
explanation
I feel that I should apologise because it's almost impossible to make a diagnosis from the appearance of that appendix. The only abnormality, apart from it being there in the first place, is a subtle nodularity with a normal overlying mucosa. perhaps this rings a faint bell ???
Actually, it turns out that the submucosa is full of small lymphoid cells clusters, forming balls. This is the classical histological appearance of a Mantle Cell Lymphoma? Mantle cell lymphoma has a predilection for the GI tract as the most common extra-nodal site. Indeed, one study found lymphoma in mucosal biopsies in 56/60 patients (both in UGI and Lower GI tract). This has given rise to a theory that mantle cell lymphoma actually originate from gut B-lymphocytes within the mantle zones of mucosal lymphoid follicles [Cancer 2003;97(3):586–91]. Endoscopic findings includes nodules, polyps, ulcers, and masses. I try to remember Mantle Cell Lymphoma if the mucosa appears markedly bumpy - as if the lymphoid follicles have gone crazy! In this case, the CT shows lots of enlarged lymphnodes, both above and below the diaphragm and the patient was started on 'Ibrutinib'. It's not a 'good lymphoma' as median life expectancy is only 6-7 yrs. This 65 yr old patient attends following EMR of an IMca for RFA WHAT WOULD YOU DO NOW? explanation
The BSG guideline as of 2013 (and updated on the topic of RFA for LGD in 2015), is very simple; RFA may be offered for flat dysplasia. The reality is often a little less clear-cut. For example, dysplastic Barrett's often appear slightly lumpy or with areas of superficial ulceration. When does a 'bumpy Barrett's' cross over into 'non-flat dysplasia'? I think that this is an example of 'not flat enough for RFA'. In fact, analysis of the original EMR specimen had reported a positive lateral margin! Expecting a local recurrence I actually went straight ahead and EMR'd the nodule which was confirmed as IMca. You will get the odd patient with Barrett's who fails to get his RFA because each time there is another little nodule to remove. Of course there are no hard and fast rules but these patients probably have 'bad disease' and are better served by an oesophagectomy. Of course, many of these are too old for surgery in which case you have no option but to keep nibbling away at their Barrett's mucosa until some adverse histological feature sends them along for chemoradiotherapy (CRT). In my experience these patients often don't do well. When chromosomal copy number analysis becomes a mainstay tool, I think that we'll see why ... This was an incidental finding in the pharynx WHAT IS THE DIAGNOSIS? explanation
This is a 'Pharyngeal retention cyst'. It was an incidental finding and the patient had no symptoms relating to this. These are the most common benign lesions in the pharynx, usually arising behind the epiglottis (the area is called the valleculae) or more to the side as here. The cysts are thought to result from dilatation of mucus glands secondary to retained secretions and chronic inflammation. They are usually incidental findings although larger cysts (>1 cm) may cause dysphagia, coughing or dysphonia. Complications include ulceration and secondary infections. During ESD, the endoscopists encounter these vessels in the rectum WHAT WOULD YOU DO? explanation
Now this looks weird. It's a video of a gastroscopy, starting just after intubation ... WHAT IS THE DIAGNOSIS? explanation
This is a patient with end-stage achalasia and a huge, 'sigmoid' oesophagus. OK, the GOJ doesn't look tight but naturally this is because the patient has in the past undergone a myotomy and fundoplication. Patients with 'Type I achalasia' presents with more severe oesophageal dilatation and less spasm-induced pain than in type II and type III achalasia. The silly question for the endoscopist was; 'is there anything we can do to improve swallowing'? Of course, a more important question for the endoscopist was: 'is there any sign of cancer in the distal oesophagus?' After all, both SCC and adenocarcinoma may develop with a frequency of about 1:700 patient/years. Which is about half as common as cancer developing in Barrett's. The GOJ looks a little plump and odd but biopsies did not reveal any neoplasia. Presumably the appearance was due to the previous fundoplication. By the way, the classification of achalasia makes no sense to me at all. This is a case of what would be called 'Type I' achalasia, which I suspect is the end stage of Type II achalasia (logically it should then be called 'Type III achalasia' shouldn't it?). The reason for the suggestion is that in 'Type II achalasia', there is still some preservation of the longitudinal muscle contraction and sufficient excitation of the circular muscle to generate intraluminal pressure but with weak forward propulsion. In type III achalasia, there is a 'nutcracker oesophagus' with a spastic gastro-oesophageal sphincter. Then again, perhaps the three subtypes of achalasia are three completely separate conditions? If you want a reminder of achalasia, here is a link to a good article! 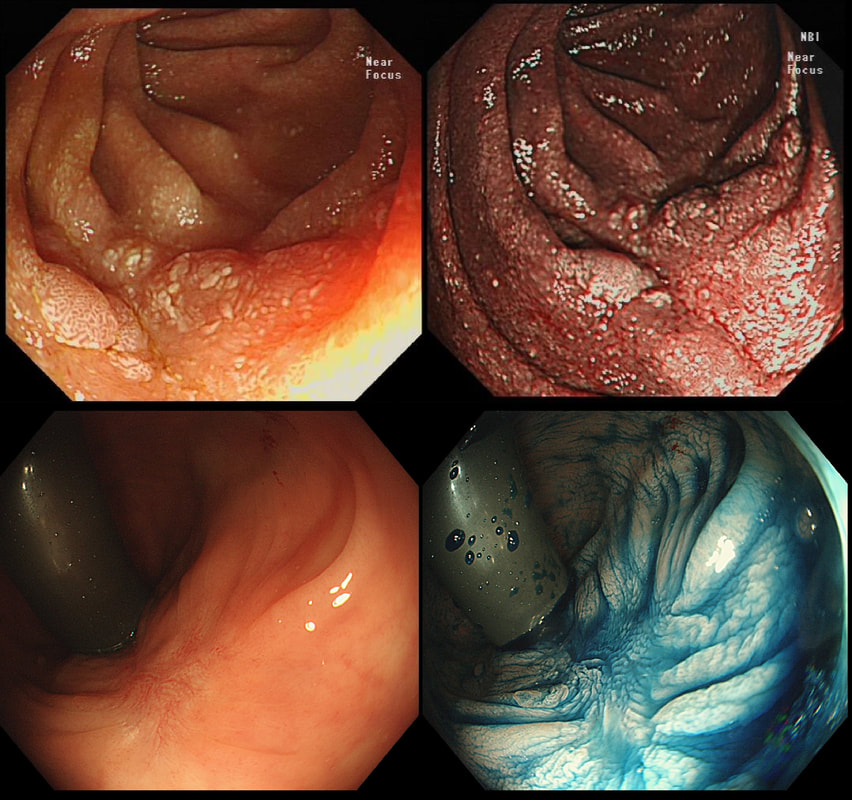
Two EMR sites. The top in the duodenum and the bottom in the rectum
ARE THE SCARS 'CLEAN'?
explanation
The teaching point behind these two images is the simple message that it's impossible to see a local recurrence with just 'white light'. You must assess the scars with NBI or dye sprye or both (I do)! In addition, remember that most local recurrences are to be find at the most 'difficult to see edge'. Perhaps you can only see a local recurrence in retrovertion?
In these particular cases both have a local recurrence (see below).

This polyp was found in the caecum.
WHAT'S THE LIKELY DIAGNOSIS?
explanation
I did hesitate for a moment as the lesion did, at first sight seem to arise from the caecal pole and was reminiscient of an inverted appendix (see below). However, on closer scrutiny, it has the typical wide-open crypts of a 'sessile serrated polyp' and wasn't actually that close the the caecal pole. It was removed without incidence after injecting some saline below.
|